| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
DERMATITIS EXFOLIATIVA1
Synonyms.—Pityriasis rubra; General exfoliative dermatitis; Acute general
dermatitis; Fr., Dermatite exfoliatrice; Erythrodermie exfoliante (Besnier).
Definition.—A more or less generalized, exceptionally limited,
exfoliating inflammatory disease of acute or subacute type and of variable
duration, arising primarily as such or supervening upon other chronic
scaly affections.
Symptoms.—As a primary affection the disease may begin in
sidiously in several scattered regions, probably more commonly (Leloir
and Vidal) about the axillae, genitocrural region, and other flexures;
it rapidly spreads, and together with the appearance of new areas soon
covers the greater part or the entire surface; or there may be at once
more or less general involvement. Exceptionally, the disease may
remain, for a time at least, more or less limited in its distribution (Crocker,
Bulkley, and others). I have met with several cases in which the chief
brunt of the process was borne by the extremities.
In many cases the outbreak is preceded by a distinct chill or chilli
ness, malaise, and sometimes vomiting and febrile action; these symp
toms may or may not continue. The skin is noted to be hyperemic
1 Important literature: Erasmus Wilson, Med. Times and Gazette, 1870, i, p. 118,
and Treatise on Diseases of the Skin; Hebra, in Hebra and Kaposi's Hautkrankheiten,
second edition, 1874, vol. i, p. 398; Hebra, Jr., Archiv, 1876, p. 508; Anderson, Brit.
Med. Jour., Dec 8, 1877, p. 812; Baxter, ibid., 1879, ii, pp. 79 and 119 (an important
paper); Jamieson, Edinburgh Med. Jour., April, 1880, p. 879; Duhring, Philada. Med.
Times, Jan. 17, 1880; Pye-Smith, Guy's Hosp. Repts., 1881, vol. xxv, p. 27; Hyde,
Chicago Med. Jour, and Examiner, Feb., 1881; Brocq, “Etude critique et clinique sur
la dermatite exfoliatrice généralisée,” These de Paris, 1882; abstract in Annales, 1883,
p. 90 (an important paper), and (pityriasis rubra), Archives Géneral de Méd., 1884, p.
550; Vidal (histology), Bull, de la Soc. Méd. des Hôpitaux de Paris, 1882, p. 101;
Mackenzie, Brit. Jour. Derm., 1889, p. 285 (an important paper—an analytic study of
21 cases); Besnier (érythrodermie) in French translation of Kaposi‘s treatise by Besnier
and Doyon, Elsenberg, Archiv, 1887, p. 727; Leviseur, Jour. Cutan. Dis., 1890, p.
482; Handford (with pigmentation), Brit. Jour. Derm., 1894, p. 241; discussion (Petrini,
Crocker, Jamieson, Brocq, Unna, Vidal, Schwimmer, Kaposi, Hebra, Jr., Besnier),
“Congrès Internat. de Derm, et de Syph.,” 1889, Comptes Rendus, Paris, 1890, pp. 43
to 80; Jadassohn, Ueber die Pityriasis Rubra (Hebra), Vienna and Leipzig, 1882, and
in Archiv, 1891, p. 941, 1892, pp. 85, 271, 462 (an exhaustive histologic and pathologic
study); Leloir and Vidal, Traitê des Mal de la Peau, 1889; W. G. Smith, Brit. Jour.
Derm., 1898, p. 437 (a succinct presentation of the subject, with a report of 2 cases),
and discussion (Payne, Galloway, Colcott Fox, Crocker, Mackenzie, Pringle, Leslie
Roberts, Whitfield, Malcolm Morris, and others), ibid., pp. 447 to 464; Morrow (fatal
in six weeks, with abscess formations), Jour. Cutan. Dis., 1898, p. 541; ibid., 1887, P-
439 (from psoriasis, and with pustular lesions—with discussion); Diehl (following
typhoid fever), ibid., p. 222; Coleman, Dublin Jour, of Med. Sci., January, 1898;
Pringle, Brit. Jour. Derm., 1899, p. 27; Burnside Foster, Jour. Cutan. Dis., April,
1907, p. 164 (13 cases—various types; among which, 4 cases of dermatitis exfoliativa
neonatorum, and 2, and possibly 3 of pityriasis rubra); Bowen, “‘Seven Cases of Der
matitis Exfoliativa with a Fatal Ending in Five,” ibid., January, 1910 (clinical, bacte-
riologic, and blood examinations; autopsy reports).
200
INFLAMMA TIONS
and red, with at first usually slight and sometimes scarcely perceptible
inflammatory infiltration; later it may become more pronounced, and
occasionally quite marked. After a short period—several days to a week
or more—the characteristic exfoliative feature presents, the exfoliation
taking place as thin, variously sized flakes or as slightly thickened imbri
cated scales. As a rule, however, the scales are thin, and usually of a
dirty gray or brownish tinge; the underlying skin is smooth, red, and
shiny, and later has a yellowish cast. The process thus instituted con
tinues, the formation of new scales going almost hand in hand with
exfoliation of the older. There are at times in some cases hyperesthesia
of the skin and a feeling of coldness. If the dermatic condition is of an
acute type, there may be accompanying febrile action, with evening
exacerbation; on the other hand, when the process is, or becomes
sluggish, there is usually slight temperature depression noted. After
a variable time—several weeks to a few months—the process begins
to abate, the skin loses its inflammatory aspect, is less red, and the
exfoliation is less marked and less rapid. Finally, the symptoms all
decline, and the malady comes to an end, complete recovery taking
place. In other cases there may be a remission for a short time,
and then a fresh exacerbation, after which, or after two or three such
remissions, recovery ensues. In other instances the disease continues,
either with or without short or long remissions, or short intermissions
almost indefinitely. In many of the cases of primary dermatitis exfolia-
tiva recovery has usually ensued after several months, and the patient
remains free for a variable time—months, a few years, or longer—and
then has another attack. In some instances, however, but probably
somewhat exceptional, recovery when once established is lasting.
In the persistent cases the patient's health usually begins to suffer,
and arthritic symptoms and internal and other complications may arise.
In these chronic and severe cases, too, the process often invades the
mucous membrane of the mouth, of the nose and conjunctiva, and may
also include that of the stomach and bronchial tubes; a cachectic condi
tion may develop. Furuncles and abscesses are sometimes superadded.
The hairs and nails are, more especially in severe continuous cases, in
volved and may be lost, and the skin becomes atrophic, tight, and limits
the movements of the joints—pityriasis rubra (Hebra). This type is
extremely rare.1
In cases evolving from psoriasis or eczema these diseases gradually,
usually after repeated or long-continued attacks, lose their special
characters, the surface, commonly in its whole extent, becomes invaded,
and there then presents the ordinary picture of an exfoliating dermatitis,
1 E. J. Stout, Philada. Polyclinic, Nov. 2, 1895, has reported a case of this type in
which there were permanent flexion of the finger-joints, nail involvement, with also
some suppurating lymphatic glands; Bowen, St. Paul Med. Jour., Feb., 1900, also
recorded a severe and persistent example of the Hebra type; this case since died of
gradual exhaustion (see Bowen's paper on the “Four Forms of Generalized Exfoliative
Dermatitis (Erythrodermies exfoliantes generalisées, Besnier),” Jour. Cutan. Dis.,
1902, p. 548; F. H. Montgomery and Bassoe have also recently (Jour. Cutan. Dis.,
1906, p. 298) reported a case with histological and autopsy findings; Gilchrist, Brit.
Med. Jour., Oct. 6,1906, has reported a case followed by peripheral gangrene of the right
hand and left foot.
DERMATITIS EXFOLIATIVA 201
in some instances with slightly more infiltration than usually observed
in cases of primary dermatitis exfoliativa.
While the typical disease is almost always erythematous in origin,
exceptionally cases have been noted in which there was some vesicula-
tion in the early stage. Occasionally, too, considerable fluid exudation
(Devergie) or a slight serous undermining, for a time at least, occurs, but
probably some of these latter cases belong more properly to the province
of pemphigus foliaceus.
The primary cases, as can be inferred, are of various grades of severity;
in rare instances of the markedly acute and hasty type grave symp-
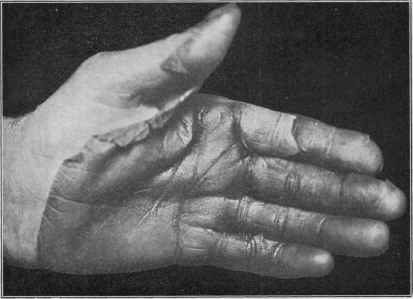
Fig. 38.—Dermatitis exfoliativa, showing the close relationship in its mildest phase,
as in this case, to erythema scarlatinoides. Patient a working-man aged twenty-five.
Four attacks in two years; practically limited to the hands, feet, and immediately
adjacent parts of the forearms and legs. Begins with burning sensation, moderate
redness, and slight swelling (this last not seen in erythema scarlatinoides), coming
on suddenly; these symptoms soon subside, and desquamation, in somewhat thick,
lamellar form, and sometimes in mass, as in the illustration, gradually presents. No
constitutional symptoms. An attack runs its course in about three weeks. There
was a suspicion in this case of drug ingestion (quinin) being the etiologic factor, sug
gested by its limited localization to the parts named, but an investigation as to the
facts of the several attacks did not confirm this.
toms of a septic character are present, and death ensues in the course
of a few weeks. On the other hand, and probably in a majority of the
cases, the disease may persist for a long time or often recur without
presenting any symptoms of an alarming character, and in some excep
tional cases, instead of being extensive, it may be, as already remarked,
somewhat limited in extent, occasionally to the hands and feet. Swell
ings of the superficial lymphatic glands have been noted (Jadassohn)
in some instances. In fact, as late analytic papers (Brocq, W. G.
Smith, Bowen) show, the disease presents itself in various types as to
202
INFLAMMA TIONS
extent and severity; the cases varying (Smith) from local forms to the
completely generalized, and from the ill-defined to the most typical.
Bowen's observations also show, as do my own, that in the division of
cases sharp lines cannot be drawn. More or less pigmentation is noted
in the recurrent and chronic cases.
The subjective symptom of itching is present to a variable degree
in almost all cases of dermatitis exfoliativa, sometimes slight, sometimes
intense; a feeling of tension and soreness or tenderness are also fre
quently complained of.
Etiology.—The disease is, as it is ordinarily met with, not con
tagious, but the infantile and epidemic varieties, which are probably
totally distinct morbid entities, and elsewhere separately considered,
are doubtless of infectious nature. The apparent etiologic or predis
posing factors are varied, and it must be conceded that the essential
cause remains practically unknown.1 Although clinically similar in
their chief external symptoms, there are doubtless several processes
etiologically considered, some of which may be accepted as of septic
and parasitic origin. The malady has been often noted to occur in
gouty and rheumatic subjects (Duckworth, Mackenzie, Crocker, and
others), and has also been seen frequently in association with tuberculosis
(Jadassohn), and in a few instances has been observed to follow excessive
alcoholism. Central or peripheral nerve changes, sometimes noted,
are suggested as having a causative relationship. On the other hand,
in some cases the patients, both preceding and at the time of the attack,
have been in fair health. As has been already stated, it sometimes
develops from a preëxisting psoriasis or squamous eczema. Local irri
tation from a drug, especially chrysarobin, arnica, mercury, and iodo-
form, has been known to provoke an outbreak in some instances; and
it is probable, too, that the ingestion of certain drugs, notably quinin, is
responsible for some of the obscure and acute attacks.
It is, fortunately, a rare disease, and observed most frequently in those
between the ages of twenty-five and sixty, and preponderantly in males.
Pathology.—In the ordinary types of dermatitis exfoliativa
various findings are recorded (Baxter, Crocker, Vidal, Jadassohn, and
others), dependent upon the character, severity, and persistence of the
disease—from a purely hyperemic condition, almost or wholly similar
to that of erythema scarlatinoides, to that in which considerable inflam
matory and atrophic changes occur. There would, indeed, seem to be a
very close relationship between the mild acute dermatitis exfoliativa and
erythema scarlatinoides.
In the extreme varieties there is a complete obliteration of the
papillae, with variable atrophy of the interpapillary rete prolongations.
The glandular structures disappear in part or wholly, and pigment
1 Tidy, in his careful analytical study (“The Metabolism in Exfoliative Derma
titis,'’ Brit. Jour. Derm. 1911, p. 133), among other facts brought out the following:
The excretion of nitrogen and fluid in the urine is deficient, and the excretion of uric
acid excessive; the excess of nitrogen and fluid is excreted by the skin; the amount of
uric acid excreted diminishes as the condition of the skin improves; the conclusion is
unavoidable that there is a direct connection between dermatitis and the amount of
uric acid excreted; the changes observed in the urine are secondary to, and a necessary
consequence of, the activity of the skin.
Plate IV.
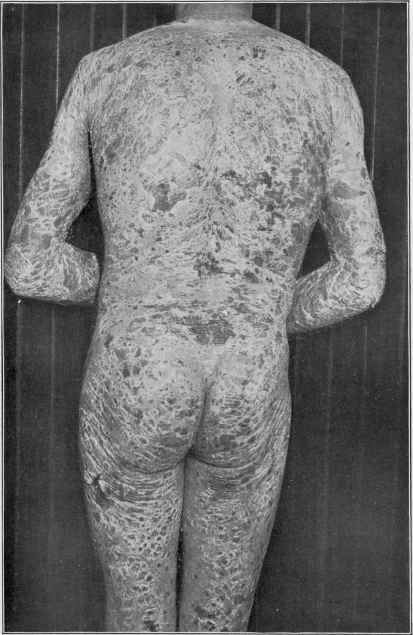
Dermatitis exfoliativa in a male adult of forty years, of eight months’ duration, fol
lowing upon a moderately extensive psoriasis of ten years’ standing. With the excep
tion of some small areas on the legs and a part of the neck, the entire surface, including
the face, was involved, with slight infiltration of the skin, and in a continuous state
of exfoliation.
DERMATITIS EXFOLIATIVA 203
granule deposit is noted in the lower epiderm, partly replacing the
rete layer. There is also sometimes noted thickening of the blood-
vessel walls in the subpapillary plexus, and both the rete and corneous
layer may be thickened, the latter irregularly, and exhibiting imperfect
keratinization. Tuberculosis of internal organs has been found in a
number of cases of the severe—pityriasis rubra (Hebra)—type.1 Myelitis
(Jamieson) and peripheral and central inflammatory nerve changes
(Quinquaud and Lancereaux) have been recorded in a few instances.
Diagnosis.—In the beginning of the process in average cases
there may be some difficulty, but a few days’ observation will usually
leave no doubt as to its nature. The exfoliative symptom, ordinarily
without systemic symptoms or throat involvement, will serve to dif
ferentiate it from scarlet fever and from erythema scarlatinoides. In
its early stage, however, in mild cases confusion with this latter malady
is possible, and in such cases, for a time at least, the disease seems to
be almost analogous. Erythema scarlatinoides is markedly acute in
character, the skin does not show the slightest or perceptible infiltration;
there may be constitutional symptoms; and, finally, its course is relatively
short, and the exfoliation frequently occurs in large, thin lamellæ and
sheets. The absence of blebs as a feature will also be an important point
of difference from pemphigus foliaceus. Psoriasis and lichen ruber,
which are also dry scaly diseases, are rarely, if ever, universal, the skin
is more thickened, and in the former the scaliness is more abundant; the
beginning papular character of the latter and the presence of typical
papules here and there at the borders of areas, even when the disease is
extensive, are sufficient to prevent error. Psoriasis may, however, as
already stated, develop into a true dermatitis exfoliativa, although such
termination is rare. In a generalized squamous eczema there will always
be found some areas in which the characteristic gummy oozing of that
disease is present; or a history of such is obtainable. Moreover, in
eczema there is usually considerable thickening and never a tendency to
thinning and atrophy.
Prognosis and Treatment.—The prognosis can be inferred from
the remarks made in describing the disease. Ordinarily idiopathic
cases with no constitutional involvement usually recover, although
some of these may succumb in future attacks. Cases with septic indi
cations are grave, and end, as a rule, fatally. The cases following on
psoriasis and eczema are persistent.
Often the disease seems to have a set course, and to be uninfluenced
by treatment. The constitutional treatment aims at removing any
possible etiologic factor, improving the tone of the general health, look
ing after the digestion, and a regulation of the bowel movements. Pilo-
1 Bruunsgaard (“Beitrag zu den tuberkulösen Hauteruptionen. Erythrodermie ex-
foliativa universalis tuberculosa,” Archiv, vol. lxvii, 1903, p. 226) reports a fatal case
with cutaneous symptoms somewhat similar to the Hebra type, but more inflamma
tory, in which tubercles were found in the papillary and subpapillary layers of the skin
and around the hair-follicles; bacilli were found in the lymph-glands, and, apparently,
it was primarily a tuberculosis of these glands, from which emboli of bacilli were carried
to the skin, producing the cutaneous inflammatory symptoms. Müller has recently
(ibid., vol. lxxxvii, 1907, p. 255) reported a case associated with tuberculous lymphatic
glands, with review of the subject and references.
204
INFLAMMA TIONS
carpin, carbolic acid, quinin, and arsenic are remedies which have been
variously advocated, but the effect is usually doubtful, and their use
requires proper caution. Mook,1 however, lauds the action of quinin,
but in large doses, from 30 to 80 gr. (2.0-4.65) daily, and the same favor
able action has been occasionally observed by Jackson,2 Hyde, and
others. Sodium salicylate and arsenic are probably most frequently of
benefit. In severe cases special efforts should be made to sustain the
strength.
The external treatment is necessary in all cases to relieve the irri
tation; beyond this its effect is questionable. Strong applications are
not only valueless, but are almost invariably damaging. Plain petro
latum, with or without 1½ to 4 grains (0.1 to 0.25) of carbolic acid to the
ounce (32.), is usually the most comforting application. In some cases
a cooling salve, as cold cream, is more grateful. Linimentum calcis is
also of service. The following mild ointment often gives considerable
relief.
R. Acid, borici, gr. xv (1.);
Acid, carbolici, gr. ij-iv (0.135-0.25);
Pulv. amyli, 3ss (2.);
Petrolati, 3j (32.).
Bran, gelatin, and starch baths are often of benefit, but should usually
be followed by an oily or ointment application. Burnside Foster found
the most satisfactory external treatment to consist in prolonged, and
when possible, continuous baths; after the former the patient being en
veloped in flannel soaked with either cod-liver oil or olive oil. Other
mild ointments and lotions, and sometimes dusting-powders, such as
prescribed in acute eczema, are also variously employed and prove sooth
ing. Engman and C. J. White3 have found in the moist cases that
continuously enveloping the patient in an abundance of dusting-powder
palliates and sometimes cures; Engman commending cornstarch powder,
and White, borated talcum, for this purpose.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |