| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
DERMATITIS MEDICAMENTOSA
451
DERMATITIS MEDICAMENTOSA1
Synonyms.—Medicinal eruptions; Drug eruptions; Fr., Eruptions médicamen-
teuses; Ger., Arznei-exantheme.
Definition.—Dermatitis medicamentosa is a term used to desig
nate all those congestive, inflammatory, and other conditions of the skin
due to the ingestion or absorption of drugs. ‘
It might well be considered also to include those cases of dermatitis
due to their external application, but the disturbance called forth by
this latter use of them is due to their direct irritant properties, and
should therefore, I believe, be classed under the head of dermatitis
venenata.
Symptoms.—The symptomatology of drug eruptions is essentially
the symptomatology of the various erythematous, exudative, and in
flammatory diseases. Thus all the various skin-lesions are encountered
in different cases, such as erythema, papules, vesicles, pustules, tubercles,
blebs, purpura, and even gangrene. The carbuncular or anthracoid
eruption and papillomatous nodules or plaques produced by iodin and
bromin compounds are, however, somewhat peculiar, and will be referred
to later when discussing each drug. In most instances there is more or
less uniformity in the type of lesion in the same individual from a par
ticular drug, but not infrequently an eruption of a mixed type may result,
such as, for example, the various symptoms of erythema multiforme.
Medicinal eruptions are apt to make their appearance somewhat
suddenly, after one or two doses, or with some drugs only after con
tinued use. They are usually highly colored. Upon withdrawal of the
drug they, with but few exceptions, as rapidly disappear. Sometimes,
however, the eruptive phenomena may continue for some time after
the drug has been stopped, as has occasionally been observed with
bromids, and less frequently with the iodids, especially in children. And
in exceptional instances it has been noted that the first appearance of
the rash has not presented until the drug had been withdrawn. Excep
tionally, too, the eruption produced may go through the various stages
of the idiopathic malady which it simulates. In generalized eruptions,
1 General literature: Behrend, “Zur allg. Diagnostik der Arzneiausschläge,” Berlin,
klin. Wochenschr., 1879, P- 714; Van Harlingen, “Medicinal Eruptions,'’ Arch. Derm.,
1880, p. 337; Morrow‘s Drug Eruptions, 1887, and the same publication with addi
tional notes and references by Colcott Fox, in Selected Monograph on Dermatology,
Sydenham Soc‘y publication, 1893; Brooke “On Behrend‘s Division of Drug Rashes
Into Specific and Dynamic Groups,” Brit. Jour. Derm., 1890, p. 313; Colcott Fox,
“Contribution to the Study of Drug Eruptions” (especially bearing upon the question
of placing eruptions due to external action of certain drugs in the same category with
the universal eruptions following internal use), ibid., p. 327; Stowers, “Drug Eruptions
—Their Nature and Varieties,” ibid., 1898, p. 289 (with discussions thereon by Payne,
Galloway, Crocker, and others, adding personal observations); Caspary, “Zur Lehre
von der Arznei-exanthemen,” Archiv, 1894, vol. xxvi, p. 11; Jadassohn, “Zur Kennt-
niss den medicamentösen Dermatosen,” Verhandl. der Deutschen dermatolog. Gesell-
schaft, V. Congress, 1895; Hudson, “Some Cases of Drug Eruptions,” Atlanta Med.
and Surg. Jour., April, 1898; Ryall, “Dermatitis Medicamentosa,” Med. Record, Dec
24, 1894. These several papers, especially those of Van Harlingen, Morrow, and
Colcott Fox, are replete with references and refer to cases to date. Pernet, “Drug
Eruptions,” Brit. Med. Jour., May 16, 1903; G. G. Campbell, “Drug Eruptions,”
Vermont Med. Monthly, Oct., 1907.
452
INFLAMMATIONS
especially of the erythematous, morbilliform, and scarlatiniform types,
there may be a variable degree of constitutional disturbance.
Etiology.—In the large majority of cases the eruption called forth
is due to some peculiar idiosyncrasy of the individual to that particular
drug, and while the same drug produces most frequently, as a general
rule, the same type of eruption in other susceptible individuals, this is
by no means always the case. On the other hand, certain few drugs,
such, for example, as the iodids and bromids, give rise so often to pus
tular or acne-like lesions that such effect may really be considered its
normal or physiologic action. Many of the more severe types of medic
inal eruption are due to the fact that the medicine is continued after
the milder manifestation has shown itself or has been administered in
large dosage; on the other hand, occasionally profound cutaneous dis
turbance results from an exceedingly small quantity.
Women and children seem to present drug idiosyncrasy most fre
quently, and those of light complexion more commonly than brunettes.
Probably, too, those of a weakened state of health and a neurotic
temperament are more susceptible than others. Defective kidney elimi
nation is certainly a factor of importance. While this peculiar idiosyn
crasy to a drug usually persists, it may in some persons entirely disap
pear; and in others small initial doses with a very gradual increase will
sometimes prevent the manifestation.
As illustrating an extreme of drug idiosyncrasy, I have had under
my observation1 a man who, upon taking an ordinary dose of quinin,
was attacked with an erythematous scarlatinoid eruption, of itchy char
acter, with some exudation, and which took several weeks to run through
its course, ending with desquamation. Several years subsequently he
went into a drug store and took a “calisaya soda-water tonic,” with the
same eruption as a result. A few years later his family physician gave
him some pills, each containing, among other ingredients, 1/16 grain dose
of quinin, of which he took only three, with the development and course
of the cutaneous outbreak as before.
Pathology.—How are drug eruptions produced? This is an in
teresting question, and as yet not conclusively settled. Three principal
theories of their action have been advanced: (I) That of skin elimination,
the drug acting as an irritant as it passes through the cutaneous tissues
or glands; (2) increased skin elimination due to defective condition of
the ordinary eliminative organs, more particularly the kidneys; (3) the
neurotic theory. The first seems plausible, but it is lacking in proof;
in fact, while it may seemingly be true with a few drugs, the weight of
investigations made proves it, upon the whole, untenable. In its support
it is claimed (Adamkiewitz, Guttmann, Giovannini) that the drug—
investigations with the iodin and bromin preparations—was found in
the sebaceous glands. This, however, as Jarisch remarks, proves nothing
unless found in greater relative quantity than in other tissues. These
findings, however, have been negatived by investigations in the same
direction (Pellizzari, Ducrez, Veiel), and also by the histologic examina-
1 Stelwagon, “ An Extraordinary Case of Quinin Susceptibility,” Jour. Cutan. Dis.,
1902, p. 13.
DERMATITIS MEDICAMENTOSA
453
tions (Thin, De Amicis, Colcott Fox, Harris, and others), which show
the first changes to be in the papillary layer, and not necessarily, except
secondarily, in or about the glands. The view (Behrend) that the pres
ence of the drug generates some toxin or irritant material in the blood
to which the eruptive phenomena are due has gained no support, but
Engman and Mook's1 investigation, while not directly in support of this,
yet are somewhat confirmatory of such a hypothesis. These investi
gations show that in ioderma and bromoderma the drug circulates in
the body tissues and which under certain conditions acts as a toxin caus
ing at points of past or present local disturbance (such as comedones,
acne lesions, seborrheic lesions, scars, traumata, scratches, etc.) all the
symptoms of an inflammation, this inflammation not differing essentially
from that produced by other toxic agents; the process consisting primarily
of inflammatory changes about the vessels. As to the second view, it is
known, it is true, that the worst forms of the iodid eruption—carbuncular
(anthracoid), bullous, nodular lesions—are seen commonly in those with
heart and kidney disease; but beyond this scanty knowledge as to the
possible causative influence of defective renal elimination, there is no
clinical evidence in its favor. The neurotic theory (Morrow), while
somewhat difficult of explanation, still has had considerable support; the
action being either purely reflex, analogous to urticaria ab ingestis, or
due to the influence of the drug upon the vasomotor centers or on the
peripheral nerves.
Diagnosis.—The diagnosis of medicinal eruptions is sometimes
difficult, but the suddenness of an outbreak should always excite sus
picion and inquiry be made. Particularly is this so with eruptions of the
nature of an exanthem. I have little doubt that many of the so-called
second attacks of the various exanthemata have been instances of drug
rashes. Medicinal eruptions seem often more violent in character than
the eruptions they simulate. As a rule, except in some of the cases of
generalized erythematous rashes, the constitutional symptoms are
rarely marked in dermatitis medicamentosa, and are not infrequently
wanting. The withdrawal of any suspected drug and one or two days’
observation will generally clear up the matter.
Treatment.—A medicinal eruption is usually to be treated ex
ternally in the same way as the eruption which it may simulate. The
carbuncular or anthracoid lesions do not need, as a rule, any operative
interference; soothing applications are generally sufficient. With
drawal of the drug is the first step, and frequently, in the milder cases
at least, nothing else is required. In others alkaline diuretics and free
drinking of water should be prescribed. In graver cases supporting
treatment is required.
With certain drugs, as, for instance, the iodid and bromids, the
coadministration of Fowler's solution (Crocker and others), potassium
1 Engman and Mook, “ A Contribution to the Histopathology and the Theory of
Drug Eruption,” Jour. Cutan. Dis., 1906, p. 502, with histologic cuts (study based upon
iodin and bromin eruptions); Pasini, Annales, 1906, p. 1, has contributed an interesting
original paper on the pathogeny of bromid eruptions; found by a special test bromin in
the lesions, but in combination with the albumin of the tissues, from which ordinary
tests could not separate it.
454 INFLAMMATIONS
bitartrate, and the maintenance of intestinal antisepsis (Féré, Eche-
verria, Gowers, Duhring) have seemed at times to have an inhibitory
action, more especially with the pustular eruptions produced by
these drugs. In fact it is probable the administration of a diuretic
along with the drug would, in some instances at least, exercise a
preventive influence. Briquet and Lyon's1 observations show that
the sodium iodid gives rise less frequently than the potassium salt
to cutaneous manifestations, and my own experience is in accord
with this.
The subject of dermatitis medicamentosa is of sufficient importance
to warrant a summary of the eruptive types provoked by different drugs
and a brief consideration of the possible eruptions which each individual
drug may produce.
The following is the summary of the forms of eruption which may
follow ingestion or absorption. Many of these drugs are capable of
giving rise to several types in different individuals or even in the same
individual; many are only rarely causative; others, such, for example,
as the bromids, iodids, quinin, copaiba, coal-tar derivatives, and others,
are somewhat frequently etiologic. To a certain extent the dividing-
line between some of the types here given is purely arbitrary and some
what ill-defined; for example, erythematopapular and polymorphous
are closely similar, but in the latter are placed those more particularly
simulative of erythema multiforme. Doubtless many more drugs will
eventually be included in this list.
Bullous.—Aconite, anacardium, antipyrin, boric acid, chloral, bro-
min, copaiba, quinin compounds, copaiba and cubebs, copaiba, iodin
compounds, iodoform, mercury, opium (?), phosphoric acid, and sali-
cylates.
Carbuncular (Anthracoid).—Arsenic, chloral, iodin and bromin com
pounds, and opium.
Cyanotic.—Acetanilid, potassium chlorate.
Edematous.—Aspirin, usually about head; salipyrin and santonin.
Eczematous.—Boric acid, belladonna, carbolic acid, opium and mor
phine, sodium borate.
Erysipelatous.—Arsenic, belladonna, conium, digitalis, ipecac, quinin,
and stramonium.
Erythematous.—Acetanilid, antipyrin, arsenic, alcohol, antitoxin,
aspirin, belladonna, benzoic acid, boric acid, bromin compounds, cap
sicum, carbolic acid, chinolin, chloral, chloralamid, cantharides, chloro
form, castor oil, conium, copaiba, copaiba and cubebs, cubebs, dulca
mara, exalgin, iodin compounds, iodoform, guaiacum, gurjun oil, hydro
cyanic acid, hyoscyamus, lead acetate, mercury, opium, pilocarpin,
piper methysticum, phenacetin, phosphoric acid, potassium chlorate,
quinin, salicylates, sodium benzoate, santonin, sodium borate, stra
monium, sulphonal, tannic acid, tar, oil of turpentine, tuberculin, vera-
trum viride, and veronal.
1 Lyon, “L'Iodisme,” Gazette des Hôpitaux, July 8, 1899—a full abstract in Jour,
mal. cutan., 1899, p. 556.
DERMATITIS MEDICAMENTOSA 455
Erythematopapular.—Acetanilid, antipyrin, benzoic acid, copaiba,
digitalis, gurjun oil, iodin compounds, iodoform, phenacetin, silver
nitrate, and potassium chlorate.
Epitheliomatous.—Arsenic (secondarily to keratoses).
Furuncular.—Antipyrin, arsenic, bromin compounds, calx sulphu-
rata, chloral, condurango, ergot, mercury, and opiates.
Gangrenous. — Arsenic,
belladonna, ergot, iodin
compounds, quinin, salicy-
lates.
Herpetic.—Arsenic, bel
ladonna, iodin compounds,
mercury, and salicylates.
Keratotic.—Arsenic.
Morbilliform. — Antipy-
rin, antitoxin, belladonna,
copaiba and cubebs, boric
acid, opium, sodium borate,
sulphonal, tar, turpentine,
tuberculin, and veronal.
Nodular. — Iodin and
bromin compounds.
Papillomatous. — Iodin
and bromin compounds.
Papular.—Arsenic, boric
acid, bromin compounds,
cantharides, chloral, conium,
copaiba and cubebs, cubebs,
digitalis, iodin compounds,
jaborandi, oil of turpentine,
mercury, terebene, and
opium.
Papulovesicular. — Cap
sicum.
Pigmentary. — Arsenic,
silver nitrate, and antipyrin.
Pruritus (Without Eruption).—Opium, chloral, copaiba, strychnin.
Purpuric (Including Petechial).—Antipyrin, antitoxin, arsenic, ben-
zoic acid, calx sulphurata, chloral, chloroform, copaiba, copaiba and
cubebs, ergot, hyoscyamus, iodoform, iodin compounds, lead acetate,
mercury, phosphoric acid, potassium chlorate, oil of sandalwood, quinin,
salicylates, stramonium, and sulphonal.
Polymorphous (Resembling Erythema Multiforme).—Antipyrin,
antitoxin, sodium benzoate, copaiba and cubebs, iodin compounds,
iodoform, boric acid, chloral, exalgin, coal-tar derivatives, opium, potas
sium chlorate.
Psoriasiform.—Sodium borate and tuberculin.
Pustular.—Aconite, antipyrin, arsenic, bromin compounds, calx
sulphurata, condurango, antimony, hyoscyamus, iodin compounds,
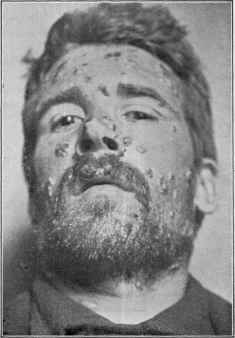
Fig. 113.—Dermatitis medicamentosa of pus-
tulobullous type, following ingestion of potassium
iodid. Principally upon the face, with some pus
tular lesions on the neck and shoulders. Sub
sided upon withdrawal of the drug, and brought
out again by experimental readministration.
456 INFLAMMATIONS
ergot, mercury, nitric acid, cod-liver oil, opium, tanacetum, oil of tur
pentine, salicylates, and veratrum viride.
Papulopustular.—Bromin and iodin compounds.
Scarlatiniform.—Antipyrin, antitoxin, belladonna, chloral, copaiba
and cubebs, copaiba, digitalis, hyoscyamus, mercury, nux vomica,
opiates, oil of turpentine, pilocarpin, rhubarb, quinin, strychnin, sul-
phonal, salicylates, stramonium, tuberculin, viburnum prunifolium, and
veronal.
Ulcerative.—Arsenic (secondarily to keratoses), brornin compounds,
chloral, iodin compounds, and mercury.
Urticarial.—Alcohol, antimony, anacardium, antipyrin, antitoxin,
arsenic, bromin compounds, benzoic acid, chloral, copaiba, copaiba
and cubebs, digitalis, dulcamara, hydrocyanic acid, guarana, hyoscya-
mus, iodin compounds, opium, mercury, pilocarpin, phenacetin, pimpin-
ella, quinin, salicylates, salol, santoninum, oil of turpentine, sodium ben-
zoate, tannin, tar, and valerian.
Vesicopustular.—Antimony, antipyrin.
Vesicular.—Aconite, anacardium, antimony, antipyrin, arsenic,
bromin compounds, cannabis indica, calx sulphurata, chloral, copaiba
and cubebs, copaiba, cod-liver oil, ergot, iodin compounds, iodoform,
nux vomica, oil of turpentine, opium, quinin, salicylates, and sodium
santonate; veronal, and other drug erythematous and erythematopapular
erruptions sometimes present some associated vesiculation, especially
on the extremities.
Hair Loss.—Boric acid and thallium acetate.
A study of the literature of the various drug eruptions, together
with personal observation of many cases, gives the following data,
briefly stated:
Aconite.—Not common; usually vesicular, exceptionally bullous, and
pustular.
Acetanilid.—Occasional; erythematous, and erythematopapular; not
infrequently cyanosis, especially of lips, face, and extremities.
Alcohol.—Rare; erythematous, and urticarial, of generalized dis
tribution.
Anacardium.—Rare; urticarial, vesicular, and bullous.
Antimony—Tartar Emetic.—Uncommon; urticarial, and vesicopus-
tular.
Antipyrin.1—Not uncommon; usually morbilliform, occasionally
erythematopapular, polymorphous, scarlatiniform, and urticarial; there
may be considerable sweating, variable pruritus, and desquamation may
follow; trunk, flexures, and occasionally face are the most common sites;
1 Apolant, “Die Antipyrinexantheme,” Archiv, 1898, vol. xlvi, p. 345 (a thorough
exposition of the subject, with brief résumé of the most important type-cases, and with
a bibliography of 265 references to date); Fournier (3 cases “Verge noire”), Annales,
1899, p. 371; Wechselmann, Deutsche med. Wochenschr., 1898, No. 21, p. 335, and
Archiv, 1899, vol. 1, p. 23; Deas (bullous), Brit. Jour. Derm., 1899, p. 194; Barthélemy
et Rellay (bullous), Annales, 1899, p. 478; Mibelli, Giorn. ital., 1897, fasc 5 and 6, pp.
575 and 697—abstract in Annales, 1898, p. 590; Bruck, Berlin, klin. Wochenschr.,
Oct. 17, 1910, No. 42, records aphthae developing on lips and tongue after a dose of
antipyrin.
DERMATITIS MEDICAMENTOSA
457
mouth, hands, and feet may also share in the eruption; exceptionally
vesicopustular, bullous, furuncular, and purpuric. The erythemato-
papular may leave behind redness and pigmentation for several weeks.
Exceptional blackness of the skin of the penis ('‘Verge noire” of the
French) has developed, usually taking a long time to disappear.
In some instances a tolerance is soon established, and the eruption
may fade while patient still continues to take the drug.
Antitoxin.1—Rather frequent; simple erythema, scarlatiniform, mor-
billiform, urticarial, and polymorphous. The morbilliform and the
scarlatiniform may or may not be followed by desquamation. There
may be prodromic symptoms, or the outbreak may be sudden, with
considerable temperature elevation, and pain and swelling about the
joints. The rash may appear shortly after the injection is admin
istered, or not until several or more days later. The subjective symp
tom of itching is variable in the different cases. The eruption lasts
usually from several days to a week or more. Exceptionally petechiæ
are observed.
Arsenic.2—Somewhat rare; almost every form of cutaneous eruption
has resulted from the internal use of this drug—erythematous, papular,
vesicular, urticarial, pustular, petechial, erysipelatous, herpetic, furun-
cular, carbuncular pigmentary, keratotic, ulcerative, and gangrenous.
1 Dubreuilh, Annales, 1895, p. 891; Hartung, Jahrbuch für Kinder heilkunde, Bd.
xliii, 1897, p. 72—full abstract in Archiv, 1900, vol. lii, p. 411 (in 375 cases, in 20 was
local irritation, and in 68 general eruption); Schulze, “Die Serumexantheme bei Diph-
therie,” Inaug. Dis., Berlin, 1898—brief abstract in Archiv, 1900, vol. lii, 19, 315 (out of
704 cases, 144 showed eruption; of these, 29 per cent, urticarial, 31.9 per cent, scarla-
tinoid, ii.i per cent, morbilliform, 20 per cent, indeterminate, and remainder not
noted); Berg, Med. Record, June 18, 1898, p. 865; Bauer (abstract with discussion),
Monatshefte, 1899, p. 450; Rawlings, St. Bartholomew's Hosp.Jour., Dec, 1898, p. 40;
Washbourn, Guy's Hosp. Gaz., Aug. 19, 1899; Malherbe, Jour. Mal. Cutan., 1904, p. 499
(“verge noire”).
2Menéau, “Les dermatoses arsenicales,” Annales, 1897, p. 345 (full paper and
bibliography of 124 references); Brouardel, “Etude sur l'Arsenicisme,” These de Paris,
Feb. 17, 1897 (an exhaustive paper); Moreira, “Arsenical Affections of the Skin,”
Brit. Jour. Derm., 1895, p. 378 (8 cases—various types); Rasch, “Contribution a
l‘etude des dermatoses d‘origine arsenicale” (2 cases, 1 zoster and 1 bullous, and partial
review of the general literature of arsenic eruptions), Annales, 1893, p. 150.
Zoster eruption: Gerhardt, Charitê-Annalen, Berlin, 1894; Nielsen, Monatshefte,
1890, vol xi, p. 302 (10 cases, with literature references to others); Bettmann, Archiv,
1900, vol. li, p. 203 (1 case and bibliography); see also under Herpes Zoster for additional
references.
Keratosis (palms and soles): Pringle, Brit. Jour. Derm., 1891, p. 390; S. Mac
kenzie (also general cutaneous pigmentation), ibid., 1896, p. 137; Colcott Fox, ibid.,
1893, p. 51; Hardaway, ibid., p. 304; Payne, ibid., 1895, p. 249; Hamburger (also
cutaneous pigmentation), Bull. Johns ‘Hopkins Hosp., April, 1900, p. 87; Boeck,
Monalshefle, 1893, vol. xvii, p. 184; Mibelli, Lo Sperimentale, 1898, Heft iv; Lang,
Annales, 1898, p. 480; Ullmann, ibid., p. 481; Arning, Verhandlungen der Deutsch.
Dermatol. Gesellschaft, V. Congress, 1894, p. 581; and Dubreuilh‘s “Kératose arsenicale
et Cancer arsenical,” report and review (Annales, Feb., 1910, p. 65) of both arsenical
keratosis and arsenical cancer (with references).
Keratosis with epitheliomatous development: Hutchinson, J. C. White, Hebra, Jr.,
Hartzell, Schamberg, and others—see Hartzell's paper, “Epithelioma as a Sequel of
Psoriasis, and the Probability of Its Arsenical Origin,” Amer. Jour. Sci., Sept., 1899;
and Debreuilh (loc. cit.), and Wile (case report, with review and résumé, and bibliog
raphy) collected 19 cases, Jour. Cutan. Dis., 1912, p. 192.
Pigmentation: Pringle, Brit. Jour. Derm., 1895, p. 52; Schlesinger, Wien. klin.
Wochenschr., 1895, p. 779; Smetana, Wien. med. Wochenschr., 1897, p. 903; Audry,
Annales, 1896, p. 1415; Müller, Archiv, 1893, vol. xxv, p. 165.
458 INFLAMMATIONS
The genital region, especially the scrotum, is the usual site of the ulcera-
tive, edematous, and gangrenous manifestation. Herpes zoster has been
observed in a number of instances to follow its administration (see Herpes
Zoster). The long-continued use of the drug, as in psoriasis and chorea,
is sometimes followed by extensive pigmentation, especially about the
trunk. As a rule, it eventually disappears sooner or later after the drug
has been discontinued. Thickening of the horny part of the skin of the
palms and soles, and over the elbows and knuckles, especially of the
hands and feet, is occasionally noted in long-continued administration.
The horny formations may undergo epitheliomatous degeneration (re
ferred to under Psoriasis and Epithelioma), and in a few instances death
has finally resulted; in fact, it is believed by several observers that the
arsenic is directly responsible for the epitheliomatous development—and
is now sometimes spoken of as “arsenical cancer.”

Fig. 114.—Keratosis (palms and soles) from the long-continued administration of
arsenic. (Another illustration showing the development of epithelioma, apparently
upon an arsenical keratosis, will be found under Epithelioma.)
Aspirin.—Somewhat exceptional; erythematous, plain or multiform;
edematous condition of face and scalp with rarely edema of the mouth
and throat also.
Belladonna—Atropin.1—Not infrequent, especially in children; scar
latinous type most usual; patchy erythematous areas or flushings occa
sional. The eruptions are, as a rule, upon suspending the drug, of short
duration. Exceptionally erythema and gangrene of scrotum have been
observed. Itching is sometimes troublesome.
Benzoic Acid and Sodium Benzoate.—Uncommon; from benzoic
acid, erythematous, erythematopapular, and urticarial, the last most
usual. After sodium benzoate, erythematous, polymorphous, and
urticarial, with or without furfuraceous desquamation.
1 Knowles, “ Generalized Eruptions of an Unusual Type, Caused by the Absorption
from a Belladonna Plaster and from the Ocular Instillation of Atropin,” Amer. Jour.
Med. Sci., July, 1911.
DERMATITIS MEDICAMENTOSA
459
Boric Acid and Sodium Borate.1—Rare; from boric acid, erythema-
tous, papular, and bullous. An inflammatory scaly eruption, eczema-
tous in character, quite marked on scalp, face, and neck, with more or
less complete loss of hair, has resulted in a few instances after long-
continued dosage; condition subsided after discontinuance and hair grew
in again. From sodium borate, rare, erythematous, morbilliform, ec-

Fig. 115.—Dermatitis medicamentosa in a young child, from the ingestion of
potassium bromid; the lesions of a pustulopapillomatous character, and of somewhat
general distribution, but most numerous and marked on the face and lower extremities
(courtesy of Dr. G. T. Jackson).
zematous, and psoriasiform eruptions, the last after prolonged adminis
tration.
Bromin Compounds.2—Quite common. An acne-like papulopustu-
lar and pustular, about the regions of the face and shoulders and back
most frequently; although the lesions are usually discrete, several or
1 Wild (boric acid and sodium borate), Lancet, 7, 1899, p. 23, with review of litera
ture; Fordyce (boric acid), Jour. Cutan. Dis., 1895, p. 499; Gowers (sodium borate),
Lancet, Oct. 24, 1884; Evans (boric acid), Brit. Med. Jour., Jan. 28, 1899.
2 Crustaceous and papillomatous eruptions: Jackson (2 cases (1 child)), Jour.
Cutan. Dis., 1895, p. 462; Elliot (2 cases—infants), Trans. Amer. Derm. Assoc.for 1895;
Panicbi, Giorn. ital., 1897, fasc 5, p. 559—abstract in Annales, 1898, p. 395; Malherbe
(vegetative and ulcerative). La Presse médicale, May 24, 1899, p. 243; Hallopeau et
Trastour (suppurating plaques), Annales, 1900, p. 883; Feulard, “Bromisme Cutanée,”
ibid., 1891, p. 531; Pini (Bromoderma nodosum fungoides), Archiv, 1900, vol. lii, p. 164,
with 4 plates—3 histologic and some literature references; Colcott Fox, Brit. Jour.
Derm., 1892, p. 287; see also paper by Van Harlingen, loc. cit.; Hall (confluent pustular,
child, with illustration), Quarterly Med. Jour., Nov., 1902, p. 138; Myers, Jour. Cutan.
Dis., 1904, p. 231 (with illustration); Hallopeau and Vielliard (gangrenous), Annales,
1904, p. 442; Parkes Weber (granuloma-like or mycotic type; case demonstration),
Brit. Jour. Derm., 1905, p. 63; Pasini, “Sur la pathogenie des eruptions bromiques”
(with review and bibliography), Annales, 1906, p. 1 (papulopustular, discrete, and
confluent); Knowles, “Unusual Cases of Bromid Eruption in Childhood,” New York
Med. Jour., March 20, 1909 (4 cases; brief review and full bibliography); Jordan,
“Ueber Bromoderma,” Dermatolog. Wochenschr., April 13, 1912, liv, p. 453, classifies
and describes various types of bromid-eruptions; records 2 severe cases, one tuberose-
and one acne-like and nodular, with some nodular groups; Halle and Dorlenscourt,
Bull. d. la Soc. de Pediat. de Paris, Feb., 1912, No. 2, p. 37, report an instance of a giant
papulotubercular bromid eruption.
460
INFLAMMATIONS
more may tend to group and become in places confluent, forming a slug
gish, conglomerate patch studded with pustular points, and bearing slight
resemblance to a superficial carbuncle. The eruption may be in some
instances more or less generally distributed. Occasionally erythematous,
vesicular, papular, urticarial, furuncular, and carbuncular eruptions
are observed to follow its administration. Exceptionally an eruption
somewhat similar to erythema nodosom is encountered. Bullous de
velopment is rarely observed.
A rather rare manifestation, occurring especially in children and
adolescents, consists of one or several or more red or purplish-red ele
vated, papillomatous, or condylomaform areas, sometimes crusted, and

Fig. 116.—Bromid eruption resembling blastomycosis and tuberculosis verrucosa
produced by ammonium bromid; disappeared slowly after its discontinuance; patient
an epileptic (Stelwagon-Gaskill Jefferson Hospital case).
sometimes presenting numerous points of pustulation; there may also
be, in parts of such lesions, superficial ulceration, but rarely of marked
character. Such formations are usually of sluggish appearance, and
while they may be numerous and of general distribution, there may be
but one or two plaques present, occupying an area of several square
inches. In the latter the lower part of the leg is the most common
site; in the extensive form, legs, arms, and region of face are favorite
situations.
Bromin eruptions (bromoderma) may ensue after a few and small
doses, but more commonly after the drug has been given for a few
weeks or longer and after large doses. Bromin eruptions have been
DERMATITIS MEDICAMENTOSA
46l
seen in infants suckled by a mother taking the drug, and when even
herself free from any manifestation.
Contrary to observation concerning most drugs, the eruptive dis
position from bromids may persist, especially in children, for several
weeks after the drug has been discontinued. The plaque or condylo-
maform type is usually slow in disappearing.
Calx Sulphurata.—Not common; usually furuncular and pustular,
rarely vesicular, and exceptionally petechial.
Cannabis Indica.—Exceptional; vesicular, more or less general, with
accompanying pruritus.
Cantharides.—Rare; erythematous and papular.
Capsicum.—Rare; erythematous and papulovesicular.
Chinolin.—Not infrequent; erythematous; observed in 6 out of 20
fever patients to whom this drug was given.
Chloral.—Not uncommon; scarlatinous most frequent and usually
accompanied with febrile action, congestion of buccal and conjunctival
mucous membranes, and followed by desquamation. Occasionally
urticarial, papular, and vesicular, and exceptionally bullous, furuncular,
carbuncular, petechial, and ulcerative; and in children, ulcers of the
tongue and cornea.
Chloralamid.—Exceptional; punctate erythematous, with vesicles,
and with redness of nasal and oral membranes, coryza, febrile action,
and subsequent desquamation.
Chloroform.—Not infrequent; erythematous, punctate, or blotchy;
exceptionally purpuric
Cod-liver Oil.—Rare; vesicular and acneiform.
Condurango.—Rare; acneiform and furuncular.
Conium.—Uncommon; erythematous, papular, and erysipelatous.
Copaiba and Cubebs.—Not infrequent; usually erythematous,
scarlatinous, morbilliform, or polymorphous; rarely vesicular, papular,
bullous, urticarial, and petechial. There may be considerable
pruritus.
Copaiba.—Not infrequent; most of the rashes observed from the
conjoint administration of copaiba and cubebs are due to this drug;
scarlatiniform, urticarial, erythematous; rarely, vesicular, petechial,
and bullous.
Cubebs.—Rather unusual; erythematous and small papular.
Digitalis.—Exceptional; scarlatiniform, papular, erythematopapular,
urticarial, and erysipelatous (of face).
Dulcamara.—Rare; erythematous, urticarial, and erythematosqua-
mous.
Ergot.—Rare, and usually only after prolonged administration.
Vesicular, petechial, pustular, furuncular, and gangrenous; this last on
the extremities and usually circumscribed.
Guarana.—Rare; urticarial.
Guaiacum.—Exceptional; miliary erythematous.
Gurjun Oil.—Rare; erythematous and erythematopapular.
Hyoscyamus.—Occasional; most commonly erythematous and urti-
carial, with edema, exceptionally scarlatiniform, pustular, and purpuric.
462
JNFLAMMATIONS
Iodin and its Compounds (Usually the Iodid Salts).1—Common;
usually the papulopustular and pustular—iodid acne, so called. This
is generally seen on face, shoulders, and back, although it may be more
or less scattered; appears after one or more weeks’ administration, and
exceptionally after a few doses. Occasionally, in places, two or more
lesions may become confluent, as in the bromid eruption, and give rise
to a papillomatous, condylomaform, carbuncular, crustaceous, or rupial
area; they are somewhat persistent, disappearing but slowly upon dis
continuance of the drug.
Exceptionally the iodids,may provoke a multiform or polymorphous
eruption closely simulating erythema multiforme and sometimes ery-

Fig. 117.—Dermatitis medicamentosa of a bullous type, from the ingestion of
potassium iodid, in a woman aged fifty. Face, neck, forearms, and hands involved, and
the seat of considerable edematous swelling and variously sized blebs. In some parts
blebs became confluent, broke, and uncovered a superficially excoriated surface, as
shown in cut. Recovery without any scarring or other trace. Patient had a weak
heart.
thema nodosum. Urticarial eruptions are also observed; likewise
vesicular, bullous, and purpuric, although these latter only rarely.
1 Recent literature of the more severe forms of iodid eruption: Hyde, Arch. Derm.,
1879, p. 333 (bullous types; with bibliography to date and analytic table), and Jour.
Cutan. Dis., 1886, p. 253 (with references); Morrow, ibid., pp. 97 and 136; Norman
Walker (vegetating, condylomatous type), Lancet, May 12, 1892, with literature refer
ences to other cases; Fordyce (nodular 1, rupia-like 2), Jour. Cutan. Dis., 1895, p. 496;
Cannet et Barasch (pustulonodular, fungoidal—death). Arch. Gén. de Médicine, Oct.,
1896, p. 424; Malherbe (ulcerative), La Presse médicale, May 24, 1899, p. 243; Neu
mann (nodular-ulcerative, skin and mucous membrane of stomach—fatal case, uremic
patient), Archiv, 1899, vol. xlviii, p. 324, with colored plates of face and stomach
lesions; Milian (purpuric), La Presse médicale, Sept. 20, 1899, p. 193; Audry (dissemi
nated gangrene), Annales, 1897, p. 1095; O. Rosenthal (tuberous and fungoidal, illus
trations), Archiv, 1901, vol. lvii, p. 3; Hallopeau and Lebret (purpuric, bullous, and
sclerous), Annales, 1903, pp. 826 and 925; Gottheil, Jour. Amer. Med. Assoc, 1909,
vol. liii, p. 1465 (fatal hemorrhagic bullous case, with illustrations; with brief notes and
references of the hemorrhagic bullous cases reported by Morrow, Hallopeau and Lebret,
and Russell); F. C. Knowles, “Purpura Caused by the Ingestion of the Iodids,” Jour.
Amer. Med. Assoc, July 9, 1910, p. 100, report of 2 petechial cases with review and
references of recorded cases; Howard Fox, Jour. Cutan. Dis., 1911, p. 93, generalized
bullous case (case demonstration).
DERMATITIS MEDICAMENTOSA 463
The bullous may be accompanied with considerable erysipelatous red
ness and swelling, and with more or less profound constitutional dis
turbance; such lesions may be numerous, sometimes confluent, and are
most commonly seen on the face, hands, and arms. Ulcerations beneath
the lesions are sometimes observed. The bullous and more severe types
of iodin eruptions are usually seen in those with kidney and heart dis
ease. The bullous and purpuric iodin eruptions are exceptionally of
grave import, and in extreme cases a fatal issue, while not to be expected,
occasionally results.
As in bromid eruptions, the eruptive tendency may persist for some
time after the drug is discontinued, more especially in children, and rarely
it does not appear until after the cessation of the drug. Iodid eruption
has been sometimes seen in nursing infants to whose mothers the drug
was being administered. Investigations (Briquet, Lyon) tend to show
that the sodium salt is least apt to give rise to eruption. This agrees
with my experience.
Iodoform.1—Uncommon; in addition to the dermatitis and eczema-
toid eruptions produced directly by the local action of this drug, referred
to under the head of Dermatitis venenata, cutaneous manifestations
exceptionally follow its absorption, and may be erythematous, erythema-
topapular, and polymorphous, vesicular, bullous, and petechial. Serious
constitutional symptoms can also result; delirium, nephritis, and death
have been observed.
Ipecacuanha.—Exceptional; circumscribed erysipelatous patches of
more or less general distribution.
Jaborandi and Pilocarpin.—Rare; erythematous, miliary, papular,
and urticarial. Active diaphoresis.
Mercury.2—Not common; erythematous, scarlatiniform, papular,
pustular, herpetic, bullous, purpuric, furuncular, and ulcerative.
Almost all, more especially the severe forms, usually resulting from
overdosing, and are scarcely observed at the present day.
Castor Oil.—Rare; erythematous, with pruritus.
Opium—Morphin.—Not uncommon; erythematous, of scarlatini-
form, morbilliform, and polymorphous types, usually with intense itch
ing; desquamation may follow; less frequently urticarial, and excep
tionally vesicular, bullous, pustular, furuncular, and carbuncular.
Piper Methysticum.—Kava-kava, the fermented juice of this plant,
gives rise to erythematosquamous, exfoliative dermatitis.
Phenacetin.—Not common; erythematous, erythematopapular, and
urticarial.
Phosphoric Acid—Phosphorus.—Rare; bullous and purpuric.
Pimpinella.—Exceptional; urticarial.
Lead—Carbonate and Acetate.—Rare; erythematous and purpuric.
1 Colcott Fox, Brit. Jour. Derm., 1890, p. 327; Taylor, N. Y. Med. Jour., Oct. 1,
1887; Cutler, Boston Med. and Surg. Jour., 1886, vol. cxv, p. 73; Etienne et Pilon,
“Revue méd. de L‘Est,” June 1, 1895, p. 339, abstract in Annales, 1896, p. 417.
2 Gottheil, Jour. Cutan. Dis., 1911, p. 114, records a case (case demonstration) in
which intramuscular injections of mercury salicylate was followed on several occasions
by an extensive eruption of a mixed type of papulovesicular eczema and erythema
multiforme; patient had nephritic symptoms.
464 INFLAMMATIONS
Potassium Chlorate.1—Exceptional; erythematopapular, polymor
phous, cyanotic.
Quinin,2 Cinchona.—Occasional; erythematous, scarlatiniform, with
or without desquamation, most commonly; less frequently urticarial,
purpuric, vesicular, bullous, erysipelatous, and gangrenous (especially
of scrotum). In the scarlatiniform and sometimes in other types of
general distribution there may be considerable constitutional disturbance,
with marked febrile action, etc. In the desquamating cases this may be
branny, lamellar, or come off in sheets or from the hands as a partial or
complete casting. Idiosyncrasy, and not dosage, is the all-important
factor. Itching is frequently present, sometimes to an annoying degree.
In doubtful cases of sudden scarlatiniform and similar eruptions
quinin should always be eliminated as a possible etiologic factor.
Rhubarb.—Exceptional; scarlatiniform desquamative erythema.
Salicylic Acid—Salicylates.—Not common; usually erythematous,
scarlatiniform, and urticarial, with or without desquamation; rarely
vesicular, bullous, purpuric, and even gangrenous.
Salol has exceptionally also been responsible for urticarial eruptions.
Salipyrin has been credited with producing edema and loss of tissue.
Santonin and Sodium Santonate.—Exceptional; from santonin,
generalized urticarial with desquamation and edema; from sodium
santonate, vesicular.
Silver Nitrate.—Slate-colored and grayish-black pigmentation or
discoloration after prolonged use; exceptionally erythematopapular
eruption.
Stramonium.—Not common; usually erythematous and scarlatini-
form; rarely erysipelatous and purpuric.
Strychnin—Nux Vomica.—Rare; scarlatiniform, and miliaria, with
pruritus.
Sulphonal.—Occasional; most commonly erythematous and scar-
latiniform, with desquamation and accompanying pruritus; rarely mor-
billiform and purpuric.
Tanacetum.—Exceptional; varioliform.
Tannin.—Rare; erythematous and urticarial.
Tar.—Rare; erythematous, morbilliform, and urticarial.
Thallium Acetate.3—More or less complete alopecia.
1 Stelwagon, “An Erythematous Eruption from Chlorate of Potassium,” New York
Med. Record, July 21, 1883.
2 Morrow, New York Med. Jour., March, 1880 (an analysis of 60 cases—in 38,
erythematous, of scalatiniform or morbilliform type; in 12, urticarial, usually with
edema or puffiness of the face; in others papular, vesicular, or petechial); Haralamb
(erythema bullosum), Annales, Dec, 1895, p. 1048; Johnston (bullous; with literature
references to several other cases), Jour. Cutan. Dis., 1896, p. 1266; Allen (acquired
idiosyncrasy), Med. Record, 1895, vol. xlvii, p. 97; Heard (generalized erythematous,
with desquamation—from 1/8grain dose), “Trans. Acad. Med. of Pittsburg,” Philada.
Med. Jour., Oct. 28, 1899; Simpson, ibid, (similar generalized case, with general des-
quamation, including the nails); Chomatianos (erythematovesicular and erythemato-
bullous, hands and penis), La Grece médicale, 1899, N0.‘4—abstract in Amer. Jour. Med.
Sci., Aug., 1899, p. 231; D. W. Montgomery (purpuric—acquired idiosyncrasy),
Boston Med. and Surg. Jour., 1897, vol. cxxxvii, p. 646.
3 Jeanselme, Annales, 1898, p. 999; Huchard, Bull, de Acad. de Méd., March 17,
1898; Vassaux, These de Paris, July 12, 1898—abstract in Annales, 1898, p. 813 (was
valuable in sweating of phthisis, but in 34 cases hair loss occurred in 8).
SCARLATINA
465
Tuberculin.—Not common; erythematous, scarlatiniform, and mor-
billiform, with or without subsequent desquamation; exceptionally,
psoriasiform.
Turpentine, Terebene.—Occasional; erythematous, scarlatiniform,
and morbilliform; exceptionally vesicular and papular, urticarial, and
pustular. Terebene, papular, with pruritus.
Valerian.—Exceptional; urticarial.
Veratrum Viride.—Rare; erythematous and pustular.
Veronal.1—Rather uncommon; erythematous, morbilliform, or scar-
latiniform, eczematoid, with sometimes vesiculation on the extremities,
and rarely large bullæ on the mucosa.
Viburnum Prunifolium.—Exceptional; scarlatiniform, with subse
quent desquamation.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |