| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
ECZEMA
Synonyms.—Tetter; Salt rheum; Fr., Eczème; Eczéma; Ger., Eczema; Ekzem;
Eczem; Nässende Flechte; Salzfluss.
Definition.—An acute, subacute, or chronic catarrhal inflamma
tory disease, characterized in the beginning by the appearance of ery
thema, papules, vesicles, or pustules, or a combination of these lesions,
with a variable amount of infiltration and thickening, terminating either
in discharge with the formation of crusts or in desquamation, and accom
panied by more or less intense itching and a feeling of heat or burning.
Symptoms.—So protean a disease may have almost any beginning
form, and often tends to change, especially into consecutive or secondary
types—eczema squamosum and eczema rubrum. As a rule, however,
when once established, its type or predominant type is apt to remain
throughout. It may begin as one or more slightly or marked inflamma
tory erythematous areas, which soon show slight or moderate scaliness;
or, instead of dry erythematous areas, the skin shows inflammatory red
ness and swelling beset with pinpoint-sized vesicles which discharge and
form crusts; or the beginning lesions may be small papules, usually aggre-
1 An interesting paper in this connection is that by Hyde, “The Influence of Light-
hunger in the Production of Psoriasis,” Brit. Med. Jour., Oct. 6, 1906.
262 INFLAMMATIONS
gated, and often so closely packed that a confluent patch results, later
tending to scaliness or vesicular formation. The beginning lesions may
also be pustular, or become rapidly so, and dry to crusts. Not infre
quently the beginning type may be of a mixed character. These are the
several primary types of the disease,—erythematous, papular, vesicular,
and pustular,—and all eczema cases begin with the presentation of one or
other of these types or a mixture of two or more. The erythematous is
usually least likely to show lesions of other types. The papular variety
often exhibits vesicles as well, and the vesicular variety not infrequently
seropurulent or purulent lesions. And when the disease is somewhat
extensive in distribution, the several types may sometimes be found on
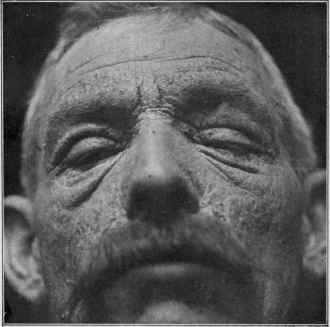
Fig. 52.—Eczema of erythematosquamous variety of several months’ duration;
deep red color; moderate scaliness; considerable thickening and infiltration, and accen
tuation of the lines and folds of the skin—this last especially marked about the eyes.
different regions. As clinically met with, a pure type, except the
erythematous, and less often the papular, is not frequently observed.
Eczema is eczema, however, whatever its variety, and the various
type names should not be allowed to confuse; type name simply signifies
the lesion or predominant lesion or condition present, and does not mean
necessarily the entire absence of other lesions or conditions; if the pre
dominance is not overwhelming, the type is usually designated mixed.
The eruption made up of an intermingling is not infrequent, and some
times the beginning of the outbreak is of ill-developed character; thus is
explained the terms erythematopapular, erythematosquamous, papulo-
squamous. vesicopapular, vesicopustular, etc. Although these are some
Plate VIII.

Eczema.
ECZEMA
263
times used to designate eruptions of mixed nature, they are more com
monly employed to signify that the lesions are of transitional or midway
character, as, for instance, the last two terms signifying that the papules
tend to vesiculation, and that the vesicles are not purely serous, but con
tain some admixture of pus, and so on. Moreover, very often the disease
does not continue as one of the beginning types, but frequently develops
into what are known as secondary or consecutive forms. Of these the
most common are eczema squamosum or squamous eczema, character
ized by moderate or marked scaliness; and eczema rubrum or eczema
madidans, characterized by a confluent, reddened, raw-looking, inflamed,
weeping surface, with crusting, but which may be at times partly or al
most completely dry. These and other types will be referred to in con
nection with the description of the lesional varieties.
The distribution of eczema may be more or less general, or, as is usu
ally the case, it may be limited to one or several regions and even to a
very small area. It may be more or less continuous in its extent, or it
may be distinctly patchy; exceptionally, as in the eczema nummulare of
Devergie, the patches may be variously coin-sized, vesicular or vesico-
papular, but usually with the margin flattening and merging into the
surrounding healthy skin. This nummular or herpetoid type occurs on
both trunk and extremities. An apparently similar or closely similar
type is that recurrent, small, rounded or ovalish patchy vesicopapular and
vesicular type more or less confined to the dorsal aspects of the hands and
forearms, with often the lesions discrete and slightly apart, as in zoster
patches and dermatitis herpetiformis; these cases are not uncommon and
are rebellious and troublesome.1 Doubtless some of these patchy cases,
especially acute in character and vesicular, usually about the hands and
feet, are due to the ringworm fungus; such, for example, as reported by
Whitfield and Sabouraud (see Ringworm).
No part of the body is exempt. At different ages different regions
show the disease much more frequently than others. Thus in infants
and young children the face and face and scalp are most usually the
seat of the malady; and in some of strumous diathesis there seems a spe
cial disposition for the eczema to be about the orifices of the mouth, ear,
nose, and eyes—its assumed association with struma leading some ob
servers to name it, without sufficient foundation, tuberculous or scrofu
lous eczema. As active working life is approached and continues, the
fingers, hands, and forearms are most commonly affected, and not
infrequently the scrotal and anal regions in the male, and the vulva in the
female; whereas in older life, past forty or fifty, the disease is seen rela
tively much more frequently on the lower part of the legs, and also
upon the face. In some cases of long-continued eczema of the fingers,
and also sometimes in association with the disease elsewhere, the nails
are observed to share in the disease; they crack and break easily, are dry
and often crumbling. The flexures of the knees, elbows, axillae, are not
infrequent sites for the eruption, and age does not seem to exercise much
influence upon the election of these regions, although these are not com-
1 Pollitzer, “A Recurrent Eczematoid Affection of the Hands,” Jour. Cutan. Dis.,
Dec, 1912, p. 716 (with illustrations), has recently reported a series of these cases.
264
INFLAMMA TIONS
mon situations in infancy and early childhood. This tendency of the
disease to affect certain parts, taken together with the age of the patient
and the chronicity, is often an important element in diagnosis.
The character of the eruption as regards the activity of the inflam
matory process may be of the acute, subacute, or chronic type. These
terms are, in eczema, somewhat confusing, inasmuch as acute and
chronic are also employed with their usual meaning in connection with
the course of the disease as regards duration. Exceptionally eczema is
observed to run an acute course, ending in several weeks or a month or
two; and in such instances the disease is almost always of a markedly
inflammatory or acute grade, and such cases are in the true sense examples
of acute eczema. As a rule, however, the course of eczema is always
chronic, and almost all cases can be classed as chronic eczema, but the
grade of the process may be acute, subacute, or chronic (sluggish) through
out.
Often the disease is of chronic type and course, with acute or sub-
acute exacerbations; in some cases it may disappear spontaneously for
a shorter or longer time, more especially in temperate or mild weather.
The subjective symptoms of eczema are almost always troublesome,
consisting of itching, burning, pricking, or stinging, or a mixture of these
several sensations; and exceptionally hyperesthesia and pain. Itching
is the most common, and is rarely missing; if so, its place is usually taken
by one of the other symptoms named. The itching may vary in degree
from slight to intense, and it may be constant or frequently intermittent.
The rubbing and scratching which it usually provokes either during full
consciousness or when asleep often have considerable influence in modi
fying the type of the disease—an erythematous or papular eczema may
be partly changed into a moist oozing form, and the vesicular, by second
ary infection, into pustular lesions.
Constitutional disturbances as a part of the disease are never ob
served except in acute generalized forms and in the acute, markedly
inflammatory and edematous eczema of the face, when there may be
preceding and accompanying febrile and other symptoms, which, how
ever, soon, as a rule, abate and disappear; followed often with a fall of
½ to 1 degree below the normal temperature. On the other hand, an
inter current febrile disease, such as typhoid, etc., usually leads to a dis
appearance of the eczema, which, however, generally recurs as soon as
the constitutional malady has run its course.
In occasional cases of eczema complications are met with, such as
blebs (rarely), furuncles, impetiginous and ecthymatous pustules, and
abscesses; these are purely accidental, and are not a part of the disease
process. They are due to accidental infection by pyogenic cocci, the
excoriations and the weakened or destroyed horny layer affording
favorable opportunities for inoculation. For the most part these lesions
are met with in debilitated subjects. Enlargement of the neighboring
lymphatic glands is also at times noted, especially in infants and young
children, and more particularly with the vesicular and pustular types,
usually the latter. In eczema rubrum of the leg, in adults, and especially
older patients, varicose veins are often seen in association and are of
ECZEMA
265
etiologic importance (eczema varicosum); in such cases there is a tend
ency, due to the same cause, to the development of leg ulcer (ulcus vari-
cosum). Other cutaneous diseases are occasionally encountered in
association with eczema or during its course, but such occurrences are
purely a matter of coincidence—eczema is in no sense protective against
other affections.
Essential Characters.—Before taking up the lesional varieties of the
disease, the essential conditions or characters of eczema, in the main to
be inferred from what has already been said, may be more distinctly
referred to. Exudation is invariable, slight in the exudative congestion
of the erythematous type, although it may also in this variety be con
siderable; more intense and often minutely circumscribed, producing
papules, vesicles, and pustules, and serous and seropurulent discharge.
There are noted also redness due to hyperemia, thickening and infiltra
tion, and often variable scaliness or crusting. There is distinct tendency
to the formation of one or more, often diffused, areas, with irregular and
ill-defined borders, the disease shading off almost imperceptibly, as a rule,
into the surrounding unaffected skin; often with, especially when about
the joints, a disposition to cracking or fissuring of the skin. It will also
be observed that fluid exudation on to the surface (eczema humidum,
moist eczema, moist tetter, salt rheum, weeping eczema), formerly
considered a sine qua non of the disease, is not always present; the parts
are often noted to be dry and scaly (eczema siccum, dry eczema, dry
tetter). To these various features are added the subjective symptoms,
of variable intensity. Several or more of these are always to be found in
every case, sometimes comparatively insignificant, sometimes pronounced.
As stated, the primary or elementary varieties are so named from
the fact that the eruption is made up of one type of lesion, or that there
is an overwhelming preponderance of such. These are also called lesional
varieties. These, as well as those of secondary or consecutive types,
deserve special description.
Eczema Erythematosum.—The most common site for erythema-
tous eczema is the face, and more especially in middle-aged and old
people. It is, however, also not infrequently met with in the flexures,
on the back of the neck, hands, and occasionally on other parts, and
exceptionally as a generalized eruption. It begins as one or more small
or large, irregularly outlined hyperemic macules or patches, pale or bright
red in color, accompanied by more or less itching and burning. At first
it may be ill defined and insignificant, but from time to time, and either
gradually or rapidly, it tends to spread, and its features to become more
pronounced; the redness becomes more conspicuous, the skin somewhat
thicker, and shows scaliness, usually branny in character, but sometimes
consisting of thin, epidermic, flake-like exfoliation. It may remain as
ill-defined patches, or, from enlargement and often the arising of new areas,
confluence takes place, and the eruption is then diffused over a part or
a whole of a region. The face is often thus involved, although not in
frequently it may be more or less limited to the forehead, and sometimes
to the region surrounding the eyes.
When the disease is fully developed, the skin is observed to be harsh
266
INFLAMMATIONS
and dry, of a reddish color, frequently with a violaceous and yellowish
tinge, and sometimes mottled; the color and inflammatory process be
coming less marked toward the healthy surrounding skin, into which the
disease merges almost imperceptibly. It is thickened, infiltrated, and
slightly scaly, with, at times, here and there, a tendency to the formation
of one or more moist or oozing areas, which are usually the result of rub
bing and scratching. In consequence of the latter, too, punctate and
linear scratch-marks and excoriations may often be seen scattered over
the affected region. In most cases, however, the whole area or region re
mains dry, and continues so throughout, with possibly, at intervals, the
appearance of provoked circumscribed oozing, which soon disappears.
The process often varies within
slight or moderate limits, becom
ing at times less pronounced, and
at others, especially after exposure
to wind or indulgence in rich food
or alcoholic stimulants, much ag
gravated. Exceptionally its course
may be acute, the disease after
several weeks tending to disap
pear; in such cases, which are,
however, rare, the face is the re
gion generally involved, and the
inflammatory process usually be
gins abruptly and is of an intense
character, the process being some
what simulative of an erysipelatous
outbreak. With few exceptions,
however, the course is chronic, al
though often fluctuating, and some
times partly abating, and occasion
ally entirely disappearing, but, as
a rule, for a short time only. Even
after complete disappearance as
the result of treatment or spon
taneously, it is exceedingly liable
to relapse, probably more strik
ingly so than is observed with the
other varieties of the disease. Very
often the scaliness becomes much
more pronounced and practically
the disease is then representative of the squamous type—eczema squa-
mosum. In rare cases, when involving the face, the eruption surround
ing the mouth, and extending outward one or more inches, is erythem-
atosquamous, with superficial furrows or cracks, sometimes in num
bers, converging toward the lips, especially to the angles; from the
effort of the patient to hold the mouth more or less fixed, to prevent
fissuring, the orificial opening seems small. Occasionally in patchy
erythematous disease about the hands and fingers, the hyperemic element

Fig 53-—Eczema of erythematosqua-
mous type, in a woman, of a year's dura
tion, involving both legs.
ECZEMA
267
is almost wanting, the eruption consisting of slight thickening, insignifi
cant scaling, and considerable fissuring. In many of these erythematous
cases, in fact, the terms erythematosquamous and fissured would be
likewise applicable.
In the flexures from friction, and the natural moisture of the parts,
the surface frequently is abraded, and a mucoid secretion, often observed
in erythema intertrigo, is noted—eczema mucosum, eczema intertrigo.
This condition is not uncommon at the scrotal, femoral, natal, and inter-
digital folds, and also under the mammæ. As already stated, however,
erythematous eczema, particularly when on the face, is apt to remain as
such, for a shorter or longer time, with, in the majority of cases, a tendency
to considerable scaliness, and thus evolving into squamous eczema. In
a few instances the skin becomes more inflamed, the surface abraded and
oozing, and often crusted, and the type known as eczema rubrum is tem
porarily or more or less permanently established. Papules, vesicles,
and pustules, lesions of the other primary types, are rarely seen in the
erythematous cases, especially those of limited distribution.
A few words should be said in regard to generalized erythematous
eczema (eczema universale), as this is the type the generalized disease
usually presents. It is rare. It begins rather suddenly, with the
appearance of small and large erythematous plaques, which rapidly
enlarge, and, together with others that form, soon result in confluence,
and practically cover the entire integument, with sometimes here and
there small free spaces. Concomitantly with the outbreak, and some
times for several hours or a day or two preceding, the patient often
feels unwell, chilly, and suffers with malaise and slight flushings of heat,
with usually slight febrile action developing. Immediately at the time
of outbreak, if acute and abrupt, there may be considerable temper
ature elevation. As a rule, such symptoms, when present, abate as
soon as the eruption has developed, but exceptionally chilliness and
febrile action, especially the latter, with evening exacerbation, may
continue for several days or longer; later, in these general cases, there
may be more or less continuous slight temperature depression. The
eruption presents the usual symptoms of the erythematous type, as
observed in the limited form, the surface being reddish, and soon slightly
branny or scaly, with often a tendency to crack aboutithe joints. Almost
always, sooner or later, on certain parts of the surface, especially on one
or more of the flexures, the moist exudation of eczema is exhibited. Itch
ing is present to a slight or severe degree, as a rule intermittently; prob
ably as troublesome a symptom is burning, and sometimes a feeling of
tension. The malady, for most of the surface at least, usually runs an
acute course, tending to disappear, sometimes after one or two exacer
bations, in several weeks to a few months, but usually leaving behind,
however, a more or less persistent involvement of one or several regions,
most commonly the lower part of the legs.
Eczema Papulosum.—Papular eczema, lichen simplex of former
authors, and sometimes called eczema lichenoides and lichen eczema-
todes, is observed most frequently upon the flexor aspects of the limbs,
although it is not uncommon upon the trunk. As with all other forms
268
INFLAMMATIONS
of the disease, it may be encountered elsewhere, but the face, ears, hands,
and fingers seldom show this variety. In my experience, in its purest
type it is more common in adults. The eruption may be sparse and
limited to a small region, or it may be more or less extensive, involving
a greater part of the integument. The lesions appear suddenly or in
sidiously, usually in numbers, and consist of discrete, aggregated, or
closely crowded reddish, pin-head-sized, acuminated, or rounded papules;
when in numbers and close together, there is often a good deal of diffused
infiltration. The aggregations, especially on the arms, often form rounded
or orbicular patches (formerly called lichen circumscriptus).
It is not uncommon, here and there, to find a variable number of
lesions so crowded that a solid patch is formed, red, inflammatory, and
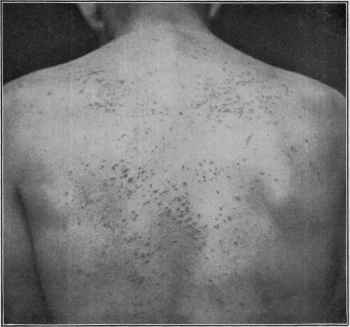
Fig. 54.—Papular eczema in male adult, of two months’ duration, limited to the back.
thickened, with usually several or more outlying discrete papules. These
patches sometimes show slight or moderate scaliness. It is not unusual,
too, for some of the papules to show slight apex vesiculation (formerly
called lichen agrius), and sometimes to develop into vesicles; and often
the latter lesions, commonly few or in moderate numbers, are found aris
ing primarily as such along with the much more numerous papules.
Occasionally the lesions are distinctly follicular in origin (eczema follicu-
lorum, follicular eczema). The papules are persistent, lasting for days
or weeks, and if disappearing, replaced by fresh lesions. In fact, often
there is a tendency to irregular appearance and disappearance, and also
to crop-like exacerbations. Sometimes the papules are minute and
punctiform in character; in other cases they are quite large to small
ECZEMA
269
pea in size, rather irregularly rounded at the base, and may be slightly
flattened on top, and when on the scrotum and lower part of the legs are
likely to be dark red or even violaceous in color, bearing some resem
blance to the larger lichen planus papules.
Papular eczema is persistent and obstinate, and usually much more
itchy than other types; excoriations, scratch-marks, and small blood-
crusts are often observed, bearing evidence of its pruritic character.
It often maintains its papular form throughout, but there is frequently
a tendency in some to become vesicles, and this tendency is, I think,
expecially observed in children. In many cases where solid patches from
overcrowding of the lesions have resulted, scaliness becomes a feature,
and the disease becomes an example of the papulosquamous or squamous
type, although it is common to find discrete papules, especially near the
periphery of the scaly area or areas; such areas are not uncommon on the
lower part of the legs. When the crowded lesions are overirritated by
rubbing and scratching, and especially if there is a tendency to vesicula-
tion, the surface becomes abraded and oozing, and eczema rubrum is
evolved.
Eczema Vesiculosum.—The vesicular variety may occur upon any
portion of the surface, but it is most usually seen upon the face of infants
and young children (crusta lactea, or milk crust, of older writers), and
in older people upon fingers and hands, neck, and flexor surfaces, especially
near the joints. As an acute outbreak it is also observed on the face of
adults. It may be limited to one region, or several regions may be
simultaneously affected, or one rapidly after the other. It is rather
rare as a widespread eruption.
It usually appears somewhat acutely, by the appearance of red
dened, more or less diffuse, patches, upon which rapidly develop numer
ous closely crowded pinpoint vesicles, rounded or acuminated, con
taining clear or slightly opaque fluid, and which tend to become pin-
head-sized or slightly larger, and so closely packed that in places practical
coalescence results. In fact, solid sheets of eruption are often thus
formed. In some cases the disease is markedly acute, and consider
able swelling and edema (eczema œdematosum), occasionally with scanty
vesiculation, are present, and when on the face, especially in adults, the
attack may at first bear resemblance to erysipelas. The vesicles soon
mature and rupture spontaneously, or are broken by rubbing or scratch
ing, and a partly vesicular and partly oozing surface ensues, on which
irregular crusting of a yellowish or honeycomb character forms. Be
neath this more or less continuous oozing takes place, and in some
places new vesicles are formed; or the disease process in the course of
days or several weeks may decline, the crusts be cast off, sometimes to
be quickly followed by a new abundant crop of vesicles, and the same
course be gone through. Later, lesions are apt to be less numerous, and
at times, instead of appearing crop-like, they appear irregularly. Scat
tered papules, vesicopapules, and exceptionally vesicopustules or pustules
are frequently to be seen mixed in with the vesicles, or more generally
about the borders of the involved areas. In some cases the discharge,
after rupture of the first outcropping of vesicles, is so profuse that new
270
INFLAMMATIONS
vesicles can scarcely be formed, and the surface remains for a time an
oozing one, with here and there scattered, imperfect vesiculation. The
eruption, when appearing and behaving as described, rarely remains long
the vesicular type, but the parts become thickened and infiltrated, the sur
face oozing and crusted, thus evolving into and constituting eczema rubrum.
In other cases the disease begins insidiously, especially when on
the fingers and hands, the lesions being scattered, with a tendency for
two, three, or more to form in close proximity; sometimes the contents
are absorbed, sometimes—and
this most frequently — the
lesions rupture or are broken,
exude, and dry over with a
thin crust, which may fall off
spontaneously, leaving healthy
skin beneath, or maybe pushed
off by new vesiculation be
neath; or, especially where
lesions are crowded together
in groups, the underlying part
becomes somewhat thick and
infiltrated, and for a time—a
day or two—the surface, after
vesicular rupture, oozes, and
constitutes a small patch of
eczema rubrum. These small
areas are similar to those aris
ing from grouped or coalescent
papules with vesicular capping.
If lesions are observed in the
palms and on the anterior as
pect of the fingers, they are
often, especially the former,
noted to be at first some
what deep seated, sometimes
milky in appearance, and
showing slight resemblance to
beginning pompholyx lesions.
In such cases, too, some of the efflorescences are clearly papular, and at
times with a few scattered seropurulent or purulent lesions instead of
pure vesicles. In other cases the entire eruption is vesicopapular; the
lesions are often readily broken or rubbed off, but they do not present
clearly formed or perceptible vesiculation. In other instances, at one
time the vesicles predominate, and at another period the papules, so that
a precise type designation is not possible. Occasionally the eruption is
mixed vesicular and pustular. Exceptionally the vesicular character
gradually disappears, leaving infiltrated areas which are persistent and
become scaly, thus going into the squamous form. This termination is,
however, exceptional—the usual one, if it takes place, is into eczema
rubrum, as already referred to.

Pig 55-—Follicular (sycosiform) eczema.
ECZEMA
271
The subjective symptoms are troublesome, but rarely so intense
as in papular eczema; a feeling of burning and tension is apt to be more
predominant than itching, although at times, and in some cases con
stantly, this latter may be present to an annoying degree. Fissur-
ing, especially at the affected joints, is sometimes in this, as in other
types, a feature of the case, but if present at all, is usually slight, and
rarely to such an extent as in other varieties. The course of the disease,
as can readily be inferred from the foregoing description, is usually
chronic, with often acute exacerbations. In exceptional cases, however,
the disease is acute both in character and its course.
Eczema Pustulosum.—Pustular eczema, known also under the name
of eczema impetiginosum, is seen most commonly on the scalp and face,
especially in children and young people, and more particularly those
who are ill nourished and strumous. In adults it is occasionally seen
about the bearded face, and on the thighs and lower part of the legs
(eczema sycosiforme). The pustular type, is, however, probably the
least common of the several varieties; although a pustular eczema of
the scalp, especially of the occipital region in girls and women, usu
ally of the dispensary class, due to pediculi, is not infrequent. It is
similar, although usually less actively inflammatory, in its symptoms
to eczema vesiculosum, with which it is sometimes associated. In fact,
there is often an admixture of both types. The lesions are either pus
tular from the start or develop from pre-existing vesicles, as a rule in
creasing somewhat in size. There is a marked tendency ordinarily
to rupturing of the lesions, the discharge drying to thick yellowish,
brownish, and sometimes greenish crusts (eczema crustosum). On the
scalp it is noted exceptionally that the lesions are so numerous and so
crowded that considerable epidermic undermining results, and the
seropurulent or purulent discharge is so profuse (eczema ichorosum) that
the denuded surface presents. The neighboring lymphatic glands are
usually considerably enlarged, especially in young subjects.
In adults there is a tendency for the pustules to be seated in or
about the hair-follicles (eczema folliculorum, eczema sycosiforme, follic-
ular eczema), to be, in fact, sycosiform, and when on the legs, they are
often scattered, although occasionally grouped. Some are distinctly
papular in the beginning. In this region, too, they are usually larger
than when on the face and scalp, and some approach the size of small
impetigo lesions. In extremely rare instances this sycosiform type
may involve the entire hairy system, being virtually a sycosis, although
with intense itching and other symptoms of eczema.
In recent years there has been a growing belief that many of the cases,
especially those in the class of vesicopustular, pustular or impetiginous
eczema, are in reality cases of infectious eczematoid dermatitis1 due to
1 Engman, “Dermatitis Infectiosa eczematoides,” Amer. Med., 1902-03, vol. iv, p.
769; Fordyce, “Infectious Eczematoid Dermatitis; Possible Influences of Anaphylaxis
in Skin Reactions,” Jour. Cutan. Dis., March, 1911, p. 129 (with illustrations; and
discussion); Bruck and Hidaka, Archiv, Feb., 1910, c, p. 165 (abstract in Jour. Cutan.
Dis., 1911, p. 188), “Biologische Untersuchungen über die Rolle der Staphylokokken
bei Ekzemen”), found that staphylococci in cases of eczema can produce biologic
reactions which consist in an increase in the agglutinins as well as the antilysin
272
INFLAMMATIONS
pathogenic pyogenic cocci. In these cases the eczematoid eruption
frequently follows or is coincident with some pyogenic process, such as
occurs in scabies, infected wounds or traumatisms, impetigo, ecthyma,
furuncles, abscesses, pus discharges, etc.
The course of pustular eczema is chronic, with exacerbations, but
not so persistently so as other varieties. The subjective symptoms
may be slight, with intermittent attacks of itching of variable degree,
or the itching may be almost constant. Soreness and burning are
also sometimes complained of.
Eczema Rubrum.—This is a secondary or consecutive type, evolving
from the primary or elementary varieties, as has been already referred
to in describing the latter. It is evolved most commonly from the
moist lesional types, but on the legs it frequently follows also the ery-
thematous form. It is a common clinical variety, and may be seen on
any part of the surface, but is not uncommon about the face and scalp
in infants and children, and quite frequent on the legs in middle-aged
and old people. It is a weeping or oozing form, but not constantly
so, and is chronic and persistent, with, as a rule, but slight variation.
Its features are considerable infiltration and thickening, often with
swelling, and sometimes with intermittent edema, and with variable
degrees of redness—not always bright red, as the name might suggest.
The surface is usually oozing, which may be slight or marked, and hence
there may be slight or considerable crusting produced from time to time;
in the markedly oozing type (eczema madidans) of the leg (weeping
leg), the surface is commonly free from any general crusting, the surface
being, as a rule, raw looking, acutely inflammatory in appearance, with
the oozing very diffused over the surface, or in the form of thickly set
minute drops. As with all eczematous oozing, it is sticky in character.
Often the exudation may lessen, and slight crusting ensue; occasionally
in these cases the exudation, though not profuse, may be seropurulent
and quite thick, and result in places in the formation of adherent, heaped-
up crusting (eczema crustosum).
In other cases the surface is free from any evident discharge, but to
the touch the surface is noted to be perceptibly moist or sticky. In other
instances, at times, even perceptible moisture is wanting, and the surface
presents a reddish, glazed appearance, being deprived of a great part or the
entire horny layer. The infiltration, thickening, redness, diffused char
acters, are, however, common to all, and exceptionally the first two may
be so considerable as to suggest mildly or moderately developed ele
phantiasis. In the cases with marked varicosity (varicose eczema, eczema
varicosum), the leg ulcer (ulcus varicosum) is not infrequently associated.
Frequently at the borders of the area, or near by, some elementary
lesions are to be observed, showing from which primary type the dis
content of the blood, and further that the chronicity and severity of the eczema
influence these antibody productions; it is evident, therefore, that staphylococci cannot
be regarded as harmless parasites in cases of eczema; Sutton, “Uber die Möglickeiten
von Verwandtscbaftsbeziehungen zwischen der Dermatitis infectiosa Ekzematoides,
der Dermatitis repens und der Acrodermatitis perstans,” Monatshefte, 1911, Band 53,
believes there is an etiologic identity in these conditions and equally influenced by
vaccine therapy (case and histologic illustrations).
ECZEMA
273
ease has evolved. The subjective symptoms, especially itching, are
usually troublesome.
Eczema Squamosum.—Squamous eczema is a not uncommon
secondary or consecutive clinical type, developing most usually, as a
chronic form, from the erythem-
atous and closely aggregated
papular types. It may, how
ever, evolve from other primary
varieties, and all these, as well
as eczema rubrum, in fact, go
through a slight or moderate
scaly stage when declining, or
during periods of lessened ac
tivity. It may be seen on any
part of the surface, but is most
frequently observed on the scalp,
back of the neck, palms, and the
legs. Other forms may also be
present, as in all the other varie
ties—for instance, on the leg,
where it often evolves from the
papular variety, where the pap
ules are closely crowded, scattered,
and aggregated; papules may be
near by or more or less remote.
It may be present as one large
area, or there may be several
patches; they are red and scaly,
with the border fading gradually
into the unaffected skin. Ex
ceptionally the areas are more or
less sharply circumscribed, and
in rare instances are somewhat
numerous; the disease picture
seems, in reality, to represent features of both eczema and psoriasis
(eczema psoriasiforme, psoriatic eczema).
There is usually a good deal of infiltration and thickening, espe
cially when it follows the papular variety. The scaliness is somewhat
variable, in some cases considerable, in others slight; and the amount
often varies materially from time to time in the same case. This is
due partly to frequency of washing, to intermittent or continuous treat
ment, or entire lack of it, as well as to the activity of the sweat secretion.
The scales are dry, thin, or massed and imbricated, in color whitish to
brownish yellow; occasionally they seem to partake slightly of the nature
of a crust, being somewhat moist or greasy, as if there had been an insig
nificant admixture of a fluid exudation, often probably oily in character
(dermatitis seborrhoica, q. v.). When about the joints, and not infre
quently on the lingers and palm, there is usually a marked tendency to
fissuring. Itching is slight or intense, and sometimes variable. This
18

Fig. 56.—Squamous eczema, with tendency
in lower part to eczema rubrum.
274
INFLAMMATIONS
variety of the malady pursues a chronic course, as, in fact, do almost all
other forms of eczema.
Eczema Fissum.—This is an important and not uncommon clinical
type, known also as fissured eczema, eczema rimosum, and eczema
rhagadiforme. It is especially common about the fingers and hands.
The conspicuous symptom is a marked tendency to fissuring or crack
ing of the skin, and usually deep in character and painful. It is com
monly a part of an erythematous or patchy squamous eczema of the
parts named, the fissuring constituting the most conspicuous and trouble
some symptom. Indeed, sometimes the skin seems scarcely reddened
or scaly, merely slightly or moderately thickened, smooth and dry,
and without scaliness; in other, somewhat exceptional cases, the skin,
especially at the finger ends, is apparently even thinner than normal, pale,
glossy, red, and atrophic in appearance, and inelastic, fissures forming
from time to time. The condition known as chapping or chaps is an
extremely mild example of the fissured variety, although such cases can
scarcely be called eczematous; more frequently, indicating a dry and
poorly nourished condition of the skin, in subjects eczematously inclined.
Eczema fissum is more or less persistent, the tendency to fissuring varying
considerably, often according to the state of the weather, frequently
disappearing spontaneously in the summer months.
Other clinical or name varieties are to be noted, due to some pecu
liarity of the disease process or to some developmental tendency. Thus,
rarely there is observed a scarcely evident erythematous type, in which
the outer epiderm shows superficial cracks, extending only to the rete, the
latter being bared, and appearing as palered or red lines, often crossing
at right angles or irregularly. In some places the epiderm, just at the
edges of the cracks, is slightly detached and may turn upward. These
thin cuticular filmy scales are quite adherent, except at the borders just
mentioned. Occasionally minute, scarcely macroscopically visible
vesiculation can be noted. The peculiar appearance is such as would
convey the impression that the outer epiderm had been too small for the
body, and that the cracking had thus resulted. It bears resemblance
also to crackled china. It is rare, usually occurring on the trunk or thighs.
It is commonly quite extensive, and is observed in neurotic subjects.
Occasionally chilliness is not unusual, especially when disrobing. Burn
ing, sometimes associated with hyperesthesia, is probably more com
plained of than itching. This variety is variously known as crackled
eczema, furrowed eczema, and eczema craquelé.
Another type of eczema—eczema sclerosum—is occasionally en
countered about the legs, especially the region of the ankle, usually
developing from the squamous type, particularly that following upon
aggregated large papules. The skin is noted to be thickened, infil
trated, hard, and almost horny, and somewhat elevated, and some
times rather sharply defined. This type is also observed in limited
patches on the palms, fingers, and on the soles. In such cases acci
dental, forcible flexing of a finger joint near or above which a patch
may be situated will cause deep fissuring. Sometimes, on the palms
and flexor surface of the fingers and also on the soles, this form of the
ECZEMA
275
disease approaches closely to tylosis or callositas, and hence the name,
eczema tyloticum. Instead of the surface of a sclerous patch, near the
ankle, being more or less flattened, it may be rough and uneven, showing
papillary hypertrophy, or crowded, wart-like projections—eczema
verrucosum. In rare instances, usually as a small area, the eruption
is moist and papillomatous and frambesiform (Beco, Huber).1
The term parasitic eczema (eczema parasiticum) is a yet somewhat
vague term; it is applied, often without sufficient reason, to those cases
of eczematous aspect in which the disease is patchy and sharply or
slightly circumscribed in outline. As a rule, however, the term is not
applied to the eczematous irritation produced by such animal para-

Fig. 57.—Eczema rubrum, of considerable duration, involving face, ears, and neck;
showing a good deal of thickening and crusting (courtesy of Dr. M. B. Hartzell).
sites as lice, fleas, etc, although it might very well be. The nummular
eczema of Devergie, and the recurrent rounded small eczematous patches
frequently seen on back of fingers, hand, and forearm, are suggestive
clinically of an active parasitic factor, but most investigations have been
negative. The ringworm fungus is known to be capable of producing
manifestations in which all the ordinary features of ringworm, except
being sharply defined and circumscribed, are absent, the patch or patches
in other respects being distinctly eczematous—usually vesicopapular,
1 J. Beco, “Uncas d‘eczéma impetigineux d‘apparence frambœsoide,” Annales de la
Societé Medico-Chirurgicale de Liege, 1894, xxxiii, p. 218; Alfred Huber, “Perifollicu-
litis suppurativa und frambœsiforme Vegetationen im Anschlusse an Ekzem” (with 2
case illustrations), Archiv, 1899, vol. xlix, P. 57.
276
INFLAMMATIONS
squamous, or of the eczema rubrum type; the genitocrural region,
axillae, hands, fingers, face, and feet, especially about the toes, are some
times the seat of such eczematoid manifestations of the ringworm fungus
invasion, as recently emphasized by the observations of Sabouraud and
Whitfield. Eczema marginatum, to be considered under the head of
Ringworm, is a typical example. Fungi other than that of ringworm have
also been found occasionally in circumscribed eczema areas, but as yet
the subject is chaotic, and alleged examples are relatively few. There
are such possibilities, however, as the occasional eczematous-looking
patches due to the ringworm fungus would indicate. Such cases are not,
I believe, judged by my own observations, so rare as commonly believed.
The designation “parasitic” is also sometimes applied to those cases illus
trative of the type known as seborrheic dermatitis (dermatitis sebor-
rhoica), which is elsewhere described.
Etiology.1—Eczema stands first in frequency among skin dis
eases for which advice is sought. It constitutes, in this country, not
less than one-third of all cases; in Europe it is much less frequent, rela
tively, at least, as other skin diseases uncommon with us are compara
tively frequent abroad. It is met with in both sexes and at all ages,
although it is probably least observed between the ages of six and fifteen.
In studying the etiology of the disease many factors must be con
sidered. The first which naturally suggests itself is the question of
heredity. Eczema can scarcely be said, without much reservation,
to be hereditary, for such evidence is lacking in a large proportion of
the cases. In many patients, however, there is an inherited tendency,
but this alone probably is never responsible, but such individuals, if
subjected to other contributory and exciting factors, will often present
the disease. Doubtless it would be more correct to state that some
individuals are born with irritable and easily excited skin, and therefore
this organ is readily susceptible to internal or external pathogenetic stim-
1 Valuable and suggestive papers bearing mainly upon etiology and pathology, some
of which also include eczema seborrhoicum: Bronson, “Eczema: Its Pathology and
Principles of Treatment,” Jour. Cutan. Dis., 1883, p. 129; Unna, “On the Nature
and Treatment of Eczema,” Brit. Jour. Derm., 1890. p. 231; “Meine bisherigen Be-
funde über den Morococcus,” Monatshefte, 1899, vol. xxix, p. 106; Bulkley, “On the
Causes of Eczema,” Med. Record, April 4, 1891; Breda; “Das Ekzem und seine Natur,”
Archiv, 1894, vol. xxix, p. 179; Hutchinson, “The Nature of Eczema,” Clinical Journal,
London, 1895, vol. vi, p. 275; Schwimmer, “Ueber die Natur des Ekzems,” Wien. med.
Wochenschr., Nos. 30, 34,1894; Bowen, “Modern Theories and Treatment of Eczema,”
Boston Med. and Surg. Jour., Oct. 10, 1895; Leredde, “Etiologie et pathologie de
l'eczéma,” Presse médicate, May 8, 1897, and “L‘origine parasitaire de l‘eczéma,”
Annales, 1899, vol. x, p. 30; L'eczéma, maladie parasitaire, Masson & Co., Paris, 1898;
Török, “L‘eczéma-est-il une maladie parasitaire?” Annales, Dec, 1898; Malcolm
Morris, “What are We to Understand by Eczema?” Brit. Jour. Derm., 1898, p. 359
(and discussion by Beatty and Colcott Fox); Leslie Roberts, “A Contribution to the
Study of Eczema,” Brit. Jour. Derm., 1899, pp. 7 and 66; Brocq, “La question des
eczémas,” Annales, Jan., Feb., and March, 1900; Sabouraud, “Essai critique sur
l‘etiologie de l‘eczéma,” Annales, April, 1899, p. 305; Galloway and Eyre, “A Study
of Certain Staphylococci producing White Cultures found in Eczema,” Brit. Jour.
Derm., Sept., 1900; Veillon, “Recherches bacteriologiques sur l‘eczéma,” Annales,
1900, p. 683; Fordyce, “The Modern Conception of Eczema,” Jour. Amer. Med. Assoc,
June 13, 1903, p. 1621; Brocq, Annales, 1903, p. 77, and Graham Chambers (etiology
and treatment), Brit. Med. Jour., Oct. 6, 1906; Johnston, “Speculations as to the
Causation of Eczema,” Jour. Cutan. Dis., Jan., 1913, p. 3 (a presentation and review
of modern theories).
ECZEMA
277
uli or excitants. It is a well-known fact that certain external irritants
will provoke a dermatitis in a large number of those exposed, whereas in
most of these it will be simply a passing dermatitis; in others—usually
a small minority—it turns out to be a true persistent eczema which has
been provoked; what this necessary something is which is present in such
individuals and not in others, and not constantly present in many of
these, is the unknown quantity in eczema of which we are still ignorant.
All that we know is that a great many factors, both constitutional and
local, have an influence in calling this “unknown quantity,'’ condi
tion, or “soil,”whatever it may be termed, into existence, of which an
inherited cutaneous irritability is, in many instances, an important one.
It has, moreover, been noted that blonde and florid persons, who are
usually apt to have dry and thin skin, belong much more numerously
in the “eczema class” than do those of dark hair and complexion; and, as
a rule, the disease is much more common in those of an active, nervous
temperament than in those of rather sluggish or phlegmatic habit. Sex
exercises but little weight, although statistics give the preponderance to
males, doubtless due to the fact that men are more subjected to ex
ternal irritants or causes. Age has but little, if any, material influ
ence, although the disease is frequent during the first several years of
life, relatively uncommon from this time to maturity, and then be
coming again frequent.
The possibility of contagiousness is a matter which requires men
tion, and which has been much discussed, but until recent years there
was but one conclusion, and that was negative, without qualification.
That is the view still predominantly held today, and is in accord with
my own experience. There are doubtless fungi and other organisms,
among which is the ringworm fungus, that are capable of giving rise to
eczematous or eczematous-looking patches, usually those of circumscribed
character, and such would naturally be communicable.
The acceptance of the presence of micro-organisms as the essential
cause of the disease—a growing belief—would naturally carry with
it the possibility of contagiousness, at least under favoring conditions,
but as yet the findings are too scanty and lacking in uniformity to
warrant such conclusion.1
The various etiologic factors of eczema can be conveniently divided
into two classes: internal, predisposing, or constitutional, and external
or exciting. Either can doubtless act independently of the other, more
particularly the external, but in a large number of cases both are necessary..
Constitutional Causes.—These are varied, and include all systemic
states or conditions, passing or persistent, which bring about impaired
or depressed vitality, and which interfere with proper nutrition, assimi
lation, and excretion. Experience has taught that gouty and rheu
matic subjects are especially liable (Bazin, Garrod, Duckworth, Bulk-
ley, Bird, Mapother, Duhring, Piffard, Whitfield, Watraszewski, and
many others) to the disease, and they seem, in some instances, almost
1 For status of this question, see interesting papers and discussion in Trans, of Sec-
tion Derm, and Syph., XIII. Internat. Med. Congress, Paris, 1900; and also other papers
already referred to.
278
INFLAMMATIONS
interchangeable—gout or rheumatism in the progenitors, the same or
eczema in those of the succeeding generation. Uric acid diathesis, or
lithemia, being a factor in many cases (gouty eczema), defective kidney
elimination, in consequence of which the overproduced uric acid is locked
up, is an added important element in such patients. It is now gen
erally, and doubtless more justly, believed that these conditions (gout
and rheumatism) have only an associated relationship, and not causa
tive—they as well as eczema often being due to the same or similar
underlying cause.
Digestive debility, dyspepsia, and its frequent accompaniment, con
stipation, must also be given a high place in discussing the causes of
the disease—in fact, in my experience stand first in importance, such
conditions often bringing on an eczematous attack in those of eczema-
tous tendency, and which responds rapidly as soon as perfect or rela
tively perfect digestion has been re-established. Important an etiologic
factor as it is in adults, it is even of greater influence in eczema of infants
and children. Diet, therefore, may be said to have an important bear
ing, not only by directly provoking digestive irregularity, but indirectly
when food is taken in excessive quantity, by overloading the system
with unnecessary supply. Faulty or incomplete metabolism, either
directly or by leading to the development of intestinal toxins, is probably
an important element in some cases.1 General debility, from whatever
cause, is sometimes the last contributing factor necessary to bring on an
outbreak. This debility may often be due to assimilative, nutritive, or
nervous influence—from overwork, physical or mental, probably more
potential when resulting from the latter. The constitutional state desig
nated struma is to be regarded (Trousseau, Sanglé, Hutchinson, Unna,
and others)2 as an important factor in some cases, especially in children.
In some cases it may be of reflex origin (Kroell, Abramitcheff, Kroch,
Eddowes, and others). To such factors may be ascribed some in
stances of eczema seen in association with dentition in infants—the
so-called tooth rash,3 although many of these cases are more likely
due to a coexistent digestive disturbance. In children, too, intestinal
parasites, doubtless both by reflex impression and direct action on the
process of digestion, seem to have at times an etiologic bearing. Like
wise, the occasionally observed etiologic agency of an adherent pre
puce indicates nerve relationship. The relation of the nervous system
to skin nutrition is, indeed, a close one, and nervous shock, hysteria,
neurasthenia, and like conditions sometimes have a direct determining
influence (Meyer, Tilbury Fox, Schwimmer, Bulkley, Duhring, Morris,
Kromayer, and others), and their existence always renders the disease
1 Johnston (loc. cit.), by a process of exclusion, reaches the opinion that “the
causation of eczema may be narrowed down to a derangement of the nitrogen metab
olism neither anaphylactic nor a defective synthesis of urea, but occurring where for
the moment biochemistry cannot demonstrate it. Color is lent to the theory by the
appearance in its course of allergic phenomena and urinary evidence of incomplete
desamidation. Perhaps the fault lies in a failure of protein—splitting in the intestinal
wall or the blood stream before the tissues select their store of amino-acid nitrogen.’‘
2 Sanglé, “Etude sur l‘eczéma scrofuleux,” These de Paris, 1880. No. 161.
3 Hall (“Etiology of Infantile Eczema,” Brit. Jour. Derm., 1908, p. 6) found that in
over four-fifths of the cases dentition had not begun when the rash first appeared.
ECZEMA
279
more rebellious. It is probably by the disturbing action on the ner
vous system that vaccination in children eczematously inclined occa
sionally provokes the disease. The presence of eczema should not,
as a rule, however, in average cases, be an obstacle to this procedure, for
experience teaches, while it is occasionally an exciting and aggravating
factor, it likewise sometimes influences the disease favorably.
Among other less active predisposing causes which indicate defect
ive kidney elimination, and which also aid in bringing about a debili
tated condition, are to be mentioned albuminuria, diabetes mellitus
(eczema diabeticorum), and diabetes insipidus—the dry skin resulting
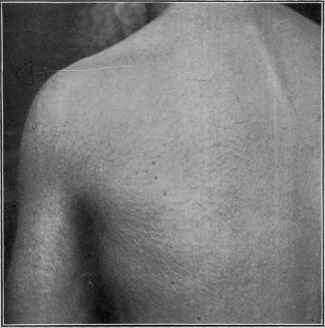
Fig. 58.—Eczema of crackled variety, in a neurotic old man past sixty, and of
several months’ duration, involving the surface more or less generally, but more espe
cially the trunk, arms, and thighs. The skin is not thickened—simply of a slightly
erythematous character, harsh and dry, with the corneous layer crackled, the fissures
superficial, disclosing the red rete.
from the last two is probably a factor of importance. Liveing1 directs
attention to the occasional presence of eczema, especially in old people,
in those with saccharine urine due usually to overfeeding without com
pensatory work or exercise and to defective assimilation, and not neces
sarily indicative of true diabetes mellitus. Functional and organic uter
ine disorders and nerve injuries (Bowlby, Cavafy, Nikolski, Brouardel,
Oulmont and Touchard, and others) have in some cases had etiologic
bearing and are additional evidences of the action of the nervous sys
tem. This frequent relationship has given rise to the term neurotic
eczema. Malarial poisoning is also occasionally an important factor.
1 Liveing, Lancet, 1881, i, p. 411.
28o
INFLAMMATIONS
Eczema certainly seems in some cases to bear relationship to the
mucous membranes; thus an association with asthma is now and then
met with, the two maladies, usually existing, getting worse and improv
ing simultaneously. Exceptionally it has been noted by some observers
that an improvement of one was followed by aggravation of the other;
such instances have rarely come under my notice. It is barely possible
that the stomachic and intestinal catarrh frequently associated with
eczema—probably a catarrhal inflammation of the skin—is in real
ity the same disease process and due to the same causes; although
the fact that the cure or relief of the digestive trouble by treatment
addressed to it alone favorably influences the skin eruption, does not
seem to support this view; on the contrary, this seems to show more
positively merely an etiologic relationship.

Fig. 59.—Eczema of thickened, sclerous, and verrucous variety, in a man aged
about thirty-five, limited to regions shown, and of several years’ duration. Deep
brownish-red color, with purplish tinge, and bearing some clinical resemblance to hyper-
trophic lichen planus patches. Previous history of eczema.
External Causes.—In a large number of cases an external factor
in the production of the disease cannot be discovered, and probably
does not exist. On the other hand, there are cases of eczema which
are persistent, owing to the fact that the external exciting cause re
mains unknown or unsuspected, but which, if finally discovered and
removed, brings about rapid recovery. All the agencies capable of
bringing on, by their local irritant or weakening action, erythema or der
matitis, referred to under these heads, are also capable, in some persons,
of provoking a veritable eczema, especially when long continued or
repeatedly acting. In most individuals, as has already been stated,
nothing more than a passing erythema or a variable dermatitis is pro
duced, and in many persons the action is, with most of such substances,
ECZEMA
28l
practically negative; in short, as before referred to, there is an unknown
something which makes some people susceptible, while others are unin
fluenced, be this heredity, depraved or perverted health, faulty metabo
lism, defective excretion, or some inherent or acquired state of the skin
itself, which may be, and probably is, a sensitization of the skin brought
about by some internal or external factor. Diseased conditions of the
skin, such as long-persistent seborrhea and ichthyosis, sometimes lead
to the complication or development of an eczema.
Among the more common external causes are to be mentioned
excessive use of water and soap, especially strong soaps, dyes and dye-
stuffs, chemical, irritants, mustard and other medicinal plasters, and
drugs; trade articles, such as sugar, flour, tobacco, pastes, polishing
materials, and the like. It is a matter, too, of common observation that
most of the causes may be acting for a long time without provoking
any irritation, when suddenly or gradually some underlying condition
supervenes or the resisting power of the skin has been finally overcome
(or the weakened skin is no longer able to protect itself against parasitic
invasion (?)), and an eczema results. This is seen over and over again
with certain occupations (so-called trade eczemas, occupational eczema,
occupational dermatoses), and, as a rule, when this vulnerability is
established, it remains more or less permanently.1 In this class, with ec
zema of the hands and sometimes the forearms, we find grocers—grocers’
itch or eczema; bakers, from flour and yeast—bakers’ itch or eczema;
washerwomen—washerwomen‘s eczema; stonecutters, bricklayers, past
ers, bookbinders, printers, dyers, chemists, surgeons (surgeons’ eczema,
surgical eczema, nurse‘s eczema, from use of antiseptics), woodworkers,
furriers, photographers, etc
Exposure to extreme cold (Hyde, Corlett),2 more especially to cold
winds, is a not uncommon external factor in some instances, and aggra-
1 Leloir, “Dermite professionnélle spécale (eczema des fileurs et varouleurs delin),”
Annales, 1885, p. 129; Blaschko, “Die Berufsdermatosen,” Deutsch. med. Wochenschr.,
1889, p. 925, and “Gewerblichen Hautkrankheiten,” Handbuch der Arbeiterkrankheiten
(Th. Weyl-Gustav Fischer, 1908); Herxheimer, “Ueber die gewerblichen Erkrankungen
der Haut,” Deutsch. med. Wochenschr., 1912, No. 1; Jacquet and Jourdanet, Annales,
1911—full abstract in Jour. Cutan. Dis., 1911, p. 564, “Etiologic Study of Occupational
Eczema”—think digestive disturbance combined with occupation causative; Fordyce,
“Occupational Skin Diseases,” Publication No. 17, A. A. L. L., New York City, June,
1912; and “Occupational Diseases of the Skin,” Med. Record, Feb. 3, 1912; Lefebre,
“Eczema of Spinners and Flax-soakers,” abstract in Brit. Jour. Derm., 1889, vol. i,
p. 140—original paper, These de Lille, 1888; Purdon, “Note on the Eczema of Bleach
ers,” Brit. Jour. Derm., 1891, p. 82; Lassar, “Das Ekzem der Chirurgen,” Dermatolog.
Zeitschrift, 1894, vol. i, p. 424; Stillmark, ibid., St. Petersburg med. Wochenschr., 1894,
p. 453; Merzbach, “Ueber Gewerbeczeme,” ibid., 1896, vol. iii, p. 161; Hall, “Derma
titis Occurring in the Silver and Electroplating Trades,” Brit. Jour. Derm., 1902, p. 121;
The external origin of eczema, particularly the occupational eczemas, based on a
study of 4142 cases, is exhaustively presented by Knowles, Jour. Cutan. Dis., Jan.,
1913, p. 11; with bibliography; who found 25 per cent, of eczema cases to be of definite
external origin. Other references to such cause will be found under “Dermatitis
venenata.”
2 Corlett, “Cold as an Etiologic Factor in Diseases of the Skin, with a Report of 14
Cases” (1 colored plate and 2 halftone cuts), Jour. Cutan. Dis., 1894, p. 457. The
cases eczematous in aspect, Dr. Corlett considers distinct from this disease and suggests
the name “dermatitis hiemalis”; and second paper, “A Recurrent Disease of the Skin
Associated with High Winds and Cold Weather,” Corlett and Cole, Amer. Jour. Med.
Sci., June, 1912, p. 710—full and detailed description, and histopathologic study, with
illustrations.
282
INFLAMMATIONS
vating in almost all cases. In fact, season often has a considerable
influence, the cold wintry windy weather materially adding to the
number of patients, whereas as summer weather approaches the disease
with many, especially if mild or only moderately developed, disappears
entirely. There are exceptions to this, for occasionally the malady is
worse in hot weather; this is more especially true of eczema in regions
where heat, perspiration, and friction are pronounced, as about the geni-
talia, anus, axillæ, etc
Exposure to heat-rays, but probably more especially to the actinic
rays, of the sun, is a source in susceptible people, sometimes producing
erythema solare, and in others, particularly if repeated, a more persistent
irritation, or eczema solare. The x-ray is also capable of calling forth

Fig. 6o.—A distinctly eczematous area of a few months’ duration, somewhat
rounded and. well defined, which might be truly called “parasitic eczema,” the ring
worm fungus was found.
an eczema-like process; as a rule, this is an evanescent affair, and scarcely
justifies the name of eczema, but exceptionally a persistent eczema re
sults.
Eczema resulting from dye-stuffs, usually anilin dyes, is not only met
with as a trade eczema, but not infrequently an eczema of the legs will
be due to the irritation from the dye in the socks or stockings, and a body
eczema is occasionally observed, explainable on a similar basis. The
material sometimes put in hatbands will provoke an eczema of the
forehead. Among such possible similar causes are to be sought an
explanation of some etiologically obscure cases. To not a few persons
the wearing of a rough woolen undergarment next the skin is not per
missible on account of the cutaneous irritation excited; this leads to
scratching, and the latter to congestion and possibly to an eczema. Mus
tard and other rubefacient plasters, stimulating liniments, and blisters
ECZEMA
283
should be used with considerable caution in those eczematously inclined,
for sometimes there results an outbreak which proves persistent and re
bellious. Eczema of the genital region in infants is often observed, and
the cause is usually to be found in the repeated wetting by the urine, as
well as from the irritant action of its products. The eczema of diabetics
of these parts, observed more especially in women, has as the immediate
exciting cause the irritating diabetic urine.
In speaking of so-called parasitic eczema, it is there stated that at
times the ringworm fungus is responsible for what clinically seems
to be, and doubtless is, an eczema; it is probable that this and other similar
fungi found from time to time by different observers may have a much
wider causative influence than is generally supposed. I have met with
several instances of persistent eczematous areas, in which the ringworm
fungus, or closely similar fungus, was found. Various micro-organisms,
as pus-cocci, morococci, and others, have been described, but, as already
stated, there has been no conclusive uniformity in the findings, and their
presence probably has no etiologic significance beyond, possibly, as with
the pus-cocci, a modification or complication of the eczematous picture.
The irritation provoked by the various animal parasites, as pediculi and
the acari scabiei, together with the resulting irritation produced by
scratching, often gives rise here and there to eczematous areas. Other
animal parasites, such as bed-bugs, fleas, and the like, in susceptible sub
jects may also be, exceptionally, etiologic factors.
Among drug irritants, which are also essentially chemical irritants,
must be mentioned, in the first place, iodoform. The sometimes un
toward action of this drug, more especially when used as a powder, is
referred to under Dermatitis Venenata. It at times not only is responsible
for a passing dermatitis, but occasionally it is the starting factor in a
most persistent eczema (iodoform eczema), and is a drug which should
never be employed in individuals eczematously inclined. Another
local application, rather frequently employed, capable of exciting the
disease, is mercurial ointment (eczema mercuriale). These and many
other drugs, as already intimated, in certain susceptible individuals,
produce either an artificial dermatitis, which usually soon passes away, or
which evolves into a true persistent eczema—the latter in those who are
especially prone to this disease. The same may in such subjects result
from so-called rhus poisoning, the dermatitis or eczema proving rebellious.
Pathology.—The investigations of most observers and the clin
ical evidence point, I believe, pretty conclusively to the catarrhal
nature of the disease—in other words, that it is a catarrhal inflam
mation of the skin. The acceptance of an inherently weak or debili
tated skin from various causes, and the action of varied pathologic
epithelial stimuli or irritants (Roberts, Brocq, Fordyce, and others),
either from within or without, or from both, best explain the disease
process. The grosser parasites, micro-organisms (Unna, Leredde), or
their products (Brockhardt, Bender, and Gerlach), thermic, actinic,
chemical, toxinic, and other irritating agents, may, therefore, be at times
contributory or even distinctly pathogenic in provoking the skin to the
reactionary inflammatory process we call eczema. Sabouraud, Török,
284
INFLAMMATIONS
Jadassohn, Neisser, and others believe the disease amicrobic, although
admitting that micro-organisms may be, as they undoubtedly are, of
import in the evolution or later changes in the morbid process. Unna
no longer holds to the specific coccus—the morococcus—which is now
generally considered to be the staphylococcus epidermalis albus. The
symptom of itching might suggest a primary nerve involvement as re
sponsible for the cutaneous phenomena, and nerve changes have occa
sionally been noted (Colmiatti, Leloir), but it is much more probable that
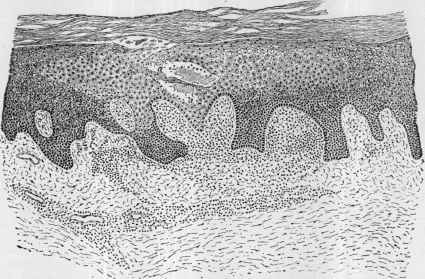
Fig. 6i.—Eczema, sluggish, deep-seated, vesicular type, with scattered lesions and
somewhat thickened corneous layer, commonly seen on the fingers; section from palmar
surface of a finger (low magnification): a, a, Represents a vesicle in the earliest ob
servable stage; the mucous layer in the lighter part shows molecular changes, and cor
responds to the area of inflammation in the papillary layer of the corium below. The
papillæ show marked serous exudation, dilated blood-vessels, and invasion of leuko
cytes (courtesy of Dr. A. R. Robinson).
this is wholly secondary. The neurotic or trophoneurotic basis of the
pathologic changes has had, however, and still has, many supporters,
as referred to when discussing etiology.
The pathologic anatomy1 of eczema has been considerably studied
1 Literature bearing upon pathologic anatomy, more especially consulted in addi
tion to that to which references were previously given: Leloir, “Contribution a l‘étude
de la formation des pustules et des vesicules sur la peau et les muqueuses” (with
bibliography), Archives de physiologie, 1880, vol. vii, p. 307; and “Contribution a
l‘étude des affections cutanées d‘origine trophiques,” ibid., 1881, vol. viii, p. 391;
“Anatomie pathologique de l‘eczéma,” Annales, 1890, p. 465; Suchard, “Des modifica
tions et de la desparition du stratum granulosum de l‘epidermis dans quelques maladies
de la peau,” Archives de physiologie, 1882, vol. ix, p. 205; Gaucher, “Note sur l‘anatomie
pathologique de l‘eczéma,” Annales, 1881, p. 263; Rindfleisch, A Manual of Pathologic
Histology, New Sydenham Soc‘y Translation, 1872, vol. i, p. 349; Neumann, Zur Kennt-
niss der Lymphgefässe der Haut des Menschen und der Säugethiere, Vienna, 1873, p. 28;
textbooks, almost all of which present cuts—Tilbury Fox, Neumann, Kaposi, Robin
son, Crocker, Jarisch, Unna ("Histopathology"), Duhring (Cutaneous Medicine, part ii),
Macleod (Pathology of the Skin),
ECZEMA 285
in recent years (Simon, Hebra, Wedl, Rindfleisch, Kaposi, Riemer,
Neumann, Biesiadecki, Robinson, Crocker, Unna, Leloir, Gilchrist,
and others). There is a difference of opinion as to whether the earliest
changes take place in the epithelium or in the papillary layer, and by
such observers that both possibilities are to be admitted. The same
difference of opinion exists as to the formation of the vesicle, its anatomic
seat being the middle or upper layers of the rete; according to investiga
tions, the earliest and most frequent formation of vesicles is within an
epithelial cell by alteration, dropsical degeneration, and expansion; and
some are formed between the epithelial cells. The pustule is a similarly
developed formation, with the addition of leukocytes. The earliest, and
possibly histologically characteristic, symptom of eczema is parenchy-
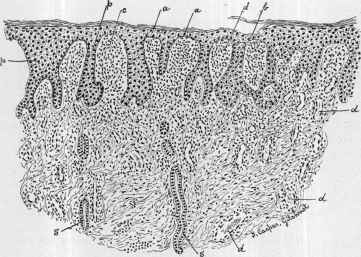
Fig. 62.—Eczema rubrum, weeping variety (low magnification): p, p, Shows
marked hypertrophy of interpapillary processes of the epiderm; a, a, thinning in some
places over the papillae, but one layer of cells at b; c, enlarged papillæ; d, d, d, d, dilated
blood-vessels; s, s, sweat-ducts, showing no change. In the corium small mononuclear
cells present in great number, with increased number of connective-tissue cells (courtesy
of Dr. T. C. Gilchrist).
matous edema of the transitional epithelium; there is, in consequence, a
broadening of the prickle layer, and these changes are noted before there is
any epithelial growth. The edema is also especially observed in the granu
lar layer, and, as a direct or indirect result, granulation ceases or is re
tarded, and proper keratinization is interfered with. The serous satura
tion of the whole epidermis, which in reality occurs, leads sooner or later
to variable epithelial growth. Along with these phenomena, or as con
tended, and probably rightly, by the majority of observers, preceding
and causing such, are to be observed a congestion and dilatation of the
vessels of the papillary layer, with consecutive diapedesis of leukocytes,
and serous exudation from the blood-vessels; in consequence the papillæ
and adjacent parts of the corium are enlarged, distended, and infiltrated,
and in some instances the deeper parts are also involved in the serous exu-
286 INFLAMMATIONS
date. In the latter cases considerable surface swelling is noted in the
more chronic disease. As a result of the epithelial proliferation referred
to, and also of the serous and cell exudation and connective-tissue cell pro
liferation, together with dilatation and engorgement of the vessels of the
upper corium, considerable thickening and infiltration ensue. In some
instances these changes are limited, primarily at least, to the follicles,
especially the hair-follicles, and are perifollicular, giving rise to papular
elevations. In those cases in which the papillæ are much enlarged and
elongated a wart-like or papillomatous aspect is given to the disease.
In acute confluent vesicular eczema and in eczema rubrum the edematous
exudation is so great and rapid as to destroy and cast off the corneous
layer, laying bare the rete.
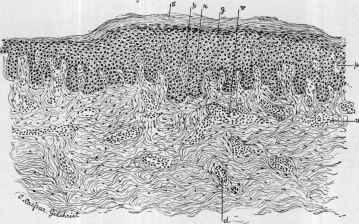
Fig. 63.—Eczema, chronic squamous variety, in a colored woman (low magnifica
tion) ; the inflammatory process involves the epidermis and upper part of the corium,
the former, especially the rete (r), being much hypertrophied, the lower half of the
corium and the glandular structures remaining practically normal: s, Scaling corneous
layer; g, granular layer; p, p, papillæ, showing but little alteration; v, v, blood-vessels
surrounded by collection of granulation-cells, numerous mast-cells, and pigment-cells;
d, part of a sweat-duct (courtesy of Dr. T. C. Gilchrist).
It will be observed from the above that the process is distinctly
an inflammatory one, with the predominance of serous exudation;
and is characterized in all cases by hyperemia, serous exudation, and
usually also by blood-vessel dilatation, epithelial and connective-tissue
cell proliferation, varying in degree according to the intensity and dura
tion of the disease; the rete and papillary layers are especially involved,
although in severe and chronic cases the lower part of the corium, and
even the subcutaneous tissue, may share in the process. The congestion
and exudation lead to increased activity of the epiderm, resulting in
scaling. In long-continued chronic eczema, especially of the legs, the
changes are still more emphasized, with pigmentation, increased thicken
ing of all parts of the affected integument, and an accentuation of the
natural lines and furrows; the papillæ, blood-vessels, and lymphatics
are considerably enlarged, and in extreme cases the sebaceous glands,
ECZEMA
287
sweat-glands, and hair-follicles suffer obliteration or degeneration, as
noted in elephantiasis.
The peculiar gummy or sticky exudation of eczema is made up chiefly
of serum and the fluid resulting from dropsical degeneration of the
rete cells. It is clear, light yellowish in color, neutral or feebly alkaline
in reaction, and deposits flocculent albumin when subjected to the usual
tests; this secretion, when dry, gives rise to the yellowish, gummy, or
candied-looking glaze or crust often observed in this malady; linen or
other material wet with it is stiffened when dry. The darker crusts of the
disease are due to the admixture of blood, pus, and dirt.
Diagnosis.—The diagnosis of eczema seems to be a field of great
difficulty to students and practitioners, and yet, if the usual features—
redness, thickening or infiltration of variable degree, the often mixed
character of the eruption, scaling or crusting, and, in many cases fluid
exudation of a sticky nature, the tendency to be confluent and to form
areas, together with the subjective symptom, itching, and the not un
common disposition to fissuring—are kept in mind, error need rarely
occur. Add to this picture a more or less chronic course, and the above
group of symptoms, in readily excluding many other diseases, becomes
almost pathognomonic. Cases seen shortly after the outbreak, thus
lacking chronicity as a feature, might be more difficult, but as the disease
often begins insidiously and slowly,—cases coming on rapidly and running
an acute course are somewhat rare,—by far the large majority do not seek
medical aid for several weeks after the onset. The value of these various
factors is still further strengthened if the favorite locations of eczema are
remembered, as the hands, face, scalp, back of the ears, genitalia, flex
ures, legs, etc. Judged by my own experience, practitioners in venturing
upon diagnosis in an untried field usually favor a rare disease rather than
a common one—if there is to be any guessing done or jumping at con
clusions, it should naturally be in the direction of the greater chances of
being right. Eczema is a frequent disease, and a large part of dermato-
logic practice is made up of its cases, and in that of the general physician
it is probably even relatively larger; the specialist's statistics of this dis
ease are apt to be reduced by the much greater number of cases of rare
diseases which naturally gravitate to him. Combining all these diagnos
tic factors,—symptoms, region, chronicity, frequency,—one is then pre
pared to say that in children under the age of four or five an itchy inflam
matory eruption of the face or scalp of any duration is usually an eczema;
the same of an eruption on the hands of a working adult; the same
of that on the leg, and to a less extent of that on the face, of the middle-
aged and old; the same of that about the genitalia and anus of a matured
adult; the same of that observed in the various flexures, etc. It is not
intended, by any means, that these statements should be taken as abso
lute, for other diseases do occur on such regions, but relatively so much
less frequently that such knowledge has value in reaching a diagnosis.
In the differential diagnosis many diseases must be considered, but
of the more common affections the most important and those most likely
to be confounded with eczema in private practice are psoriasis and sebor-
rhea, and in public practice the same and scabies, pediculosis, and im-
288
INFLAMMATIONS
petigo contagiosa. The differences between these and eczema will first
be pointed out, and then other maladies which may also at times bear
resemblance follow in alphabetic order. Among these latter those dis
eases in which itching is a factor should be more particularly considered
in the differentiation, such as pruritus, urticaria, sometimes miliaria,
and also the rarer affections, lichen planus and dermatitis herpetiformis.
Psoriasis.—Psoriasis, even though the eruption be scanty, is of more
or less general distribution: eczema is more likely to be limited to one
or two regions; psoriasis patches are variously sized, rounded, and
sharply defined: eczema is usually in one or more large, irregular areas,
and shades gradually into the surrounding skin; psoriasis favors the
extensor surfaces, especially the regions of the knees and elbows: eczema
the flexures; psoriasis lesions are uncommon upon the face and hands,
and then usually only as a part of a more or less generalized eruption,
whereas eczema is frequently seen upon these parts and often only there;
psoriasis is probably never limited to a single region, except the scalp,
and this rarely: eczema is frequently so limited; the scaliness of eczema is,
as a rule, slight: that of psoriasis, more or less abundant; eczema fre
quently shows, or gives a history of, vesicles or gummy oozing: psoriasis
is always dry; psoriasis lesions, when the scales are removed, disclose a
reddish, filmy, or membranous-looking surface, which, if scraped, shows
minute blood-drops: in squamous eczema the uncovered surface is usually
hard, thickened, and rough; psoriasis patches begin as small lesions and
increase in size by peripheral extension: scaly eczema patches, which
most resemble psoriasis, arise most frequently from overcrowding of
papules producing a solid area, and usually characteristic papules are
to be found at the periphery; in psoriasis eruption it is not uncommon
to find a few ring-shaped patches with clearing center: in eczema this
rarely, if ever, occurs. Psoriasis lesions on the palms may resemble closely
squamous eczema, but the former malady is never limited to this region,
but is seen here, and that rarely, only in conjunction with the characteris
tic areas on other parts.
Psoriasis of the scalp and squamous eczema of this region have, in
appearance, much in common, but the former is here also usually seen
as well-defined and always dry scaly patches, and eczema as more or less
diffused and sometimes in places moist; psoriasis patches are often noted
to overlap the hairy border on to the forehead and mastoid region, and if
close together, present a wavy or festooned edge, sharply defined, as
elsewhere: eczema, if it oversteps the scalp, generally does so as a diffused
eruption, fading gradually into the normal skin, and often presenting,
as it approaches the ear, especially behind the ear in the fold, moist exuda
tion; further, while psoriasis may in rare instances be limited to the scalp,
in most of the so-called scalp limitation cases usually a few insignificant
spots may be seen on the elbows and knees.
In eczema itching is practically invariable: in psoriasis it may or
may not be present; its absence would, therefore, throw the balance in
favor of psoriasis, while its presence would have but little significance,
although, as a rule, even in itchy psoriasis cases, the itching is rarely so
intense as in eczema.
ECZEMA
289
Seborrhea.—Seborrhea is sometimes confounded, but in this there is
entire absence of infiltration and thickening and of other signs of inflam
mation common to eczema; moreover, the scales of seborrhea are greasy
and oily, rather soft and unctuous to the touch, and when on non-hairy
parts, as the nose and breast, occasionally show slight prolongations into
the follicles; the underlying skin is usually pale and sluggish looking,
while in eczema, on the other hand, the scales are dry and brittle, and the
underlying skin is red, infiltrated, and often rough and hardened; often,
too, in eczema a removal of scales or crusts discloses a part of the surface
with the characteristic gummy oozing, whereas in seborrhea it is greasy
or oily. In seborrhea of the scalp, its most usual situation, if long con
tinued it is often accompanied with falling of the hair: in eczema this is
seldom noted. The itching is rarely marked in seborrhea, and sometimes
wanting, while in eczema it is more or less constant and troublesome. At
times, however, the seborrheic disease has ingrafted upon it, or appar
ently so, the eczematous process, and thus shows mildly inflammatory
symptoms; such cases are described under Dermatitis Seborrhoica, under
which the differential points of this latter from ordinary eczema will be
given.
Scabies.—The eruption of scabies is in many respects somewhat
eczematous, due to parasitic irritation, and in cases of any duration the
conditions observed in some parts, especially about the hands, in the
neighborhood of the elbow, axillae, and natal folds, may present distinct
eczematous areas. Even in such extreme cases, however, the matter of
differential diagnosis is usually readily solved. The distribution of
scabies is so characteristic as to be almost pathognomonic It is not
localized to a region or two, as eczema commonly is, but the lesions are
usually scattered and discrete, and consist often of a mixture of papules,
vesicles, small and large pustules, between the fingers, palms, and dorsum
of hands, about the wrists, region of the elbow joint, axillary folds, nipples
in women, lower abdomen, genitalia, and inner sides of the thighs, and
often on the legs and feet—a distribution and eruptive characters wanting
in eczema. Moreover, the papules, vesicles, and pustules of eczema are
small, acuminated, or rounded, those of scabies somewhat linear, and often
markedly so, and many of the lesions, especially the pustular, larger in
size. The presence of the burrow, or cuniculus, usually and most com
monly to be found on the inner sides of the fingers, and sometimes upon
the covering wall of the vesicular and pustular lesions, would be decisive.
Moreover, a history of contagion is often attainable in scabies, and fre
quently two or three members of the family are affected. In extremely
mild cases of the malady, kept so by constant bathing, and gener
ally observed in private patients, the lesions are usually ill-defined
papules, vesicopapules, and vesicles, and may be few in numbers, but
the characteristic distribution is present. Then, too, the face and scalp,
except sometimes in infants and very young children, are never involved
in scabies, and are commonly so in more or less generalized eczema.
The pruritus of scabies is most troublesome at night, and often com
paratively absent during the daytime: in eczema this difference is not
usually so marked. Scabies cannot remain limited to the region on
19
29O INFLAMMATIONS
which it first presents, but is progressive and becomes generally distrib
uted: eczema often is confined to one or two regions, and rarely is found
so generally scattered.
Pediculosis.—An eczematoid eruption of a papular, papulopustular,
and pustular character, about the scalp, especially posteriorly, and
about the pubic region, should always lead to suspicion of pediculi
as the cause; the suspicion aroused, it is an easy matter to determine
the point by the presence or absence of ova, or nits, on the hair-shafts.
This is sufficient, but the pediculi can also usually be found hidden
in the deeper meshes of the hair on the scalp, and the crab-louse on
or close to the skin, clinging to the hair in the pubic region. In addition
to the pubic region, the crab-louse also causes, but infrequently, similar
irritation about the axillae, and sometimes in other regions where there
is short hair, as in hairy individuals about the breast, legs, etc. In
extremely rare instances also an eczematous irritation of the eyelids and
of the eyebrows has been found to be due to the crab-louse on these parts,
but here, as in other situations above named, the finding of the nits
attached to the hairs will solve the problem. Pediculosis corporis, if of
long duration, and especially in the tramp class, gives rise to distinct ec-
zematous irritation, with, however, accentuation on those parts against
which the clothing comes in closest contact, as across shoulders, neck,
and upper back, around the waist, and down the outer sides of the thighs
—a distribution not observed in ordinary eczema. Even if, in many
cases, the eruptive lesions and excoriations are scanty, the same distri
bution is noted, and is usually characteristic. Then, too, parallel linear
scratch-marks of some length are more frequently noted in pediculosis
corporis than in any other itchy disease. The pediculi are often to be
found in the clothing, but unless in great numbers are usually hidden in
the seams, in which places they are to be sought for.
Impetigo Contagiosa.—It is only when impetigo lesions are close
together and coalesce, forming a crusted area, that a resemblance to
eczema is shown. Even then the nature of the lesions from which
the area resulted, as usually disclosed by the history, and also by the
presence of characteristic discrete lesions, will prevent error. The
vesicles and pustules of eczema are usually pinpoint to pin-head in
size, with tendency to spontaneous rupture; those of impetigo are
pea- to dime-sized, and exceptionally larger, and tend to dry to crusts
without breaking. In the latter disease there is often a history of
contagion.
Acne and Acne Rosacea.—Ordinarily acne can scarcely be confused
with papular or pustular eczema, as in the former disease the lesions
are always discrete, larger, and their origin from a plugging up of the
sebaceous gland outlet is usually evident. Acne rosacea with a sebor-
rheic element can show a rough resemblance, but here the hyperemia,
with no infiltration, often associated acne lesions, and the dilated capil
laries, will prevent error—such conditions are not observed in eczema;
moreover, acne rosacea is usually limited to the nose and immediate neigh
borhood: eczema, on the other hand, is apt to be diffused over the face,
and never remains limited for any length of time to the rosacea regions.
ECZEMA
291
Dermatitis.—Inflammation of the skin of artificial origin is often
similar in symptomatology to that of eczema, and may, indeed, be con
sidered identical, and therefore is to be differentiated chiefly by the
acuteness of the attack, history as to the cause, its short course and
rapid disappearance. It is also usually limited to the parts subjected
to the irritant. In many cases of artificial dermatitis the very violence
of the symptoms is suggestive. In rhus poisoning the history of exposure,
the part affected, the intensity of the process in many cases, and some
times the presence of large vesicles and blebs, would ordinarily preclude
confusing it with eczema. Rhus plants, however, like other external irri
tants, may be the exciting factor in eczema, and the violent early symp
toms give way to those of the eczematous disease; this result, fortunately,
rarely happens except in those with distinct predisposition to the latter
malady.
Dermatitis Exfoliativa.—This disease is almost invariably general
ized, and, as a rule, shows very little infiltration and thickening, and
is usually always dry and with abundant exfoliation; eczema is prac
tically never over the entire surface, but in sheets or areas, and more
marked in its favorite places, exhibits a good deal of infiltration and
thickening, slight or moderate, and often intermittent, scaliness, and
shows often, especially in the flexures, characteristic gummy oozing.
Moreover, in many cases of dermatitis exfoliativa there are symptoms
of constitutional disturbance, and in eczema such would be exceptional;
the subjective symptom of itching is much more marked in eczema, and
is usually intense, whereas in cases of dermatitis exfoliativa it may
occasionally be troublesome, but is often slight, and sometimes wanting,
the feeling being more of burning and tension. There is no doubt, how
ever, that exceptionally extensive eczema, of usually long duration, may,
as well as psoriasis, evolve into a true dermatitis exfoliativa.
Dermatitis Herpetiformis.—The cases of dermatitis herpetiformis
which could be confused with eczema are rare, and to be found only
in those cases in which the vesicular and papular lesions are small,
but in this disease the herpetic character of the eruption—the tendency
to small groups and the absence of distinct tendency to spontaneous
rupture—is different from eczema. Moreover, its variable course, with
often change of type or sprinkling of lesions of other types, as blebs, ery-
thematous and bullous rings, and other symptoms common to erythema
multiforme, is not observed in eczema.
Erysipelas.—Eczema can be mistaken for this disease only when
markedly acute, with considerable edema and swelling, but there are
sufficient points of difference. In erysipelas the character of the onset,
its method of spread usually from one point, the shining- glazed-looking
red surface, and, above all, the well-defined elevated, often as if chopped
off, border, frequently the presence of blebs, and the accompanying con
stitutional disturbance, are different from the symptoms of eczema.
In this latter there is rarely febrile action, except at the very beginning of
the acute outbreak, and this not always; the eruption often appears simul
taneously at several points, with ill-defined borders, its surface is some
times beset with minute vesicles, which usually break and discharge the
292 INFLAMMATIONS
characteristic sticky fluid, different from the serum from the broken blebs
in erysipelas. The swelling and deep-seated character of the process in
erysipelas persist until the disease has reached its acme—usually some
days: in eczema the violence of the onset generally abates within twenty-
four to forty-eight hours, and then the disease assumes the ordinary
features. Eczema is usually intensely itchy, whereas the subjective symp
toms in erysipelas are apt to be a feeling of tension, soreness, and burning,
rarely itching.
Erythema.—There is, as a rule, no difficulty in distinguishing eczema
from the various erythemata. In the milder erythemata—erythema
simplex and the other hyperemias—there is absence of distinct inflam
mation, the process being simply a congestion, though sometimes insig
nificant, scarcely perceptible exudation, but with the absence of eczema
features. Erythema intertrigo, when with a macerated surface, resembles
eczema, but the secretion is not, as that of eczema, sticky, nor does it
stiffen linen as the latter does; nor is there any infiltration. Still, ery
thema intertrigo persisting and neglected does sometimes evolve into a
true eczema. The lesions of erythema multiforme—papules, tubercles,
nodes—are much larger than those of eczema, and with little tendency to
become confluent; the erythematous patches are sharply marginate or
annular, conditions not observed in eczema. Scaliness is not noted in
the erythemata except occasionally, and then only as an almost imper
ceptible branniness or a thin filmy exfoliation; in eczema scaliness is
common and often pronounced. Moreover, the erythemata rarely itch
to any degree.
Favus.—This disease, when well defined in its earliest existence, can
scarcely be mistaken for eczema, as the yellow, mortar-like, cup-shaped
discs are pathognomonic The scalp is its usual region, and here, after
the disease has lasted for some time and been neglected, and the crusting
massed and dirty, it bears some resemblance to squamous eczema, but the
hair involvement, as shown by the dead-looking, lusterless hair, the broken
hairs, and the irregular, patchy hair loss, is never seen in the latter dis
ease. Moreover, if the crusts are removed, atrophic or scar-like tissue
is disclosed, another condition entirely foreign to eczema. In obscure or
questionable cases, which, however, are rarely met with, the microscopic
examination of the crusts will disclose the fungus if the disease be favus.
Herpes.—Herpes simplex, whether the lesions are about the lips or
face or about the genitalia, can scarcely be confused with eczema;
herpes presents a grouping of vesicles, often upon a hyperemic base, with
little, if any, disposition to spontaneous rupture: eczema vesicles are much
smaller, usually closely crowded, and generally over considerable area,
with no tendency for special grouping, and, as a rule, soon break and dis
charge a gummy fluid; the process in herpes is acute in course, disappear
ing usually in several days or one or two weeks: eczema is almost always
persistent; in herpes itching is, as a rule, absent, or so slight as to give rise
to no complaint: in eczema it is generally intense and constant. The
same reasons, with slower evolution and disappearance of the vesicles,
which are also larger, in great measure suffice to prevent confusion between
herpes zoster and eczema; moreover, the limitation of zoster to one side
ECZEMA
293
of the body or region, its appearance as erythematous and inflammatory
patches, surmounted by groups of pin-head to pea-sized vesicles, and its
distribution over the course of a nerve are entirely wanting in eczema.
Herpes zoster comes on suddenly and is often preceded and accompanied
by neuralgic pain: eczema is never neuralgic, and often insidious in its
appearance.
Lichen Planus.—The irregular base, flattened top, with often central
depression, and the dark-red or violaceous color and the glistening
surface of lichen planus papules usually suffice to distinguish them
from the rounded or acuminated, bright-red papules of eczema. The
lesions of lichen are, as a rule, slow in appearance and are persistent, and
always papules, and, when disappearing, leaving brownish or purplish
stains: those of eczema generally present acutely, and are less apt to
persist as such, often showing a tendency to vesiculation, and rarely
leave discoloration. The solid scaly areas of lichen planus resulting from
an overcrowding of the lesions bear resemblance to scaly eczema, espe
cially that evolving from papular eczema, but the lichen plaques are darker
red and usually purplish in color and sharply defined: those of eczema
bright red, and generally fade off gradually into the surrounding skin;
moreover, in lichen planus scattered, characteristic, discrete papules
are almost always to be found at the edges of the patch or near by, which
would serve for differentiation.
Lupus Erythematosus.—There is a resemblance, on casual inspection,
between squamous eczema and this disease; but in lupus erythematosus
the sharply defined border, the firmly adherent but less abundant scali-
ness, and often the evident involvement of the sebaceous glands, as shown
by the distended and scaly plugging of the ducts, and in most cases the
tendency to central atrophy of the patch, are sufficient points of differ
ence from the conditions observed in eczema, in which glandular duct in
volvement, sharp border, and atrophy are wanting. If the scales are
removed in lupus erythematosus or are scanty, the patch, pale or deep red
in color, is apt to have a dirty-white dotted look, due to the accumulation
in the ducts. Moreover, lupus erythematosus is usually a strikingly
chronic and slow process, often taking months for the formation of a dime-
or quarter-dollar-sized area. The subjective symptoms of lupus ery-
thematosus are slight or absent, whereas in eczema usually troublesome.
Ordinary eczema rarely shows the peculiar distribution common with
lupus erythematosus—across the nose, and spreading, wing-like, on to the
cheeks. When not so distributed, the above differences will, however, be
sufficient to distinguish.
Miliaria.—The vesicular variety of miliaria cannot well be mistaken
for eczema, as the lesions, though they may be numerous, are discrete
and remain so, with no tendency to confluence, and little, if any, to spon
taneous rupture, and the contained fluid is not of sticky character, fea
tures just the opposite of those observed in vesicular eczema. The
papular variety of miliaria possesses greater resemblance, but here the
discrete character, the sudden advent, and usually after profuse sweating
or heat exposure, distinguish it from papular eczema. Moreover, in
vesicular and papular eczema, when the lesions are as crowded as generally
294
INFLAMMATIONS
observed in miliaria, there are usually underlying inflammatory swelling
and perhaps infiltration, conditions not observed in the latter disease
either in its papular or vesicular varieties. Besides, eczema itches
greatly: miliaria rarely to as great a degree, and is sometimes absent, the
subjective symptoms being more a feeling of pricking, tingling, and burn
ing. Miliaria runs a rapid course, and if the cause ceases to act, disap
pears in several days to one or two weeks: eczema, although it may be
acute in coming, is apt to evolve into the chronic and persistent disease.
Pityriasis Rosea.—This malady has some resemblance to mild
scaly eczema, but the circinate tendency shown in many of its efflores
cences, the numerous patches with but slight disposition to confluence,
the superficial character of the process, its rapid appearance, and its limi
tation, in great measure, to the trunk and upper part of the limbs, the
slight degree of itching or its entire absence, and the definite course of the
disease, are characters at variance with the features and behavior of
eczema. It bears greater resemblance to dermatitis seborrhoica, under
which it will again be referred to.
Pruritus.—This disease is characterized by simple itching and noth
ing else, and, therefore, eczema, with its infiltration, vesicles, papules,
scaliness, etc., can scarcely ever be confounded with it. There is only
one symptom common to both, and that is the itching, and this, as re
marked, is the sole symptom in average cases of pruritus. In the
latter disease, however, if intense and persistent in character, the con
stant rubbing and scratching provoked may give rise to follicular papules
and some erythematous areas, but these are always in places readily
reached by the hands. Moreover, the history of pruritus, with its
absence of lesional symptoms, except those as a result of scratching, etc.,
will serve to prevent error. Pruritus ani, pruritus scroti, and pruritus
vulvæ may, however, from the incessant scratching and rubbing, lead to
true eczema.
Ringworm.—The ordinary round patch with the clearing center
of ringworm of the non-hairy surface is not met with in eczema. Nor is
the method of its spread, beginning usually as a small scaly spot, often
soon afterward with a somewhat elevated and scaly or papular or vesico-
papular border, and clearing up centrally, leaving slight scaliness or
branny furfuraceous desquamation or a smooth surface, ever seen in
eczema; this latter never behaves that way. Ringworm of the scalp may
suggest a mild scaly eczema, but in the former the evident hair involve
ment, as shown by the broken-off hairs and hair stumps, and partial
hair loss on the patch, and the insignificant scaliness are never found in
the latter malady. In the more inflammatory pustular or papulopus-
tular ringworm of this region the appearances simulate eczema, but the
hair symptoms, as described, are present and serve to differentiate.
Even in obscure disseminated scaly spots of scalp ringworm in which the
alopecia and hair invasion are not so obvious, still broken hairs and short
small stumps just peeping out from the follicles (black-dot ringworm)
suffice to distinguish it from eczema.
Ringworm of the genitocrural, and sometimes axillary, region assumes
an eczematous aspect, and has been well called “eczema marginatum,”
ECZEMA
295
but the sharply defined spreading, often festooned, border, with usually
one or several outlying typical ring-like patches, as well as the history of
the eczematous-looking area, beginning in similar ring-like manner, are
entirely different from ordinary idiopathic eczema. Moreover, in a large
majority of ringworm cases a history of contagion is elicited. Nor does
ringworm itch, as a rule, nearly so much as eczema, although the last-
named type frequently does. Occasionally an eczematoid eruption due
to the ringworm fungus is, however, observed about the hands and
toes. In doubtful cases microscopic examination of the scrapings will
determine. The differences from ringworm of the bearded region will
be considered under the next heading.
Sycosis.—There is a similarity in the eruptions of eczema and sycosis
vulgaris, but eczema is not often follicular, and the lesions are often
crowded together, forming a solid sheet; it rarely is limited to the hairy
parts of the face, but oversteps these regions, and is also often seen else
where upon the surface at the same time; the itching is troublesome.
In sycosis, on the other hand, the lesions are always follicular and dis
crete, with each lesion pierced by a hair, and even when crowded, show
their follicular character; the eruption is strictly limited to the hairy
parts, and the subjective symptoms are rarely complained of. In eczema,
moreover, there is at times apt to be the characteristic gummy discharge,
whereas this is not observed in sycosis.
In ringworm sycosis (tinea sycosis) of the superficial type the ring
patches are characteristic, and serve to differentiate from eczema.
In the deeply seated or nodular ringworm sycosis there is usually a
history of the disease beginning as a ring-like spot, the hairs are in
volved, are broken or are loosened and fall out, and there is marked
cutaneous and subcutaneous lumpiness or nodules—symptoms which
are entirely lacking in eczema.
Syphilis.—Syphilitic eruptions can rarely be confounded with
eczema. The secondary eruptions of syphilis are usually discrete,
though more or less generalized in distribution; there is no tendency
to the formation of confluent areas; they are darker in color, and more
sluggishly inflammatory in appearance, and the color does not always
disappear upon pressure, as commonly in eczema; and, in addition, there
are other symptoms of syphilis, and often a history or evidence of the
initial lesion; moreover, eczema itches, and the syphilodermata do not,
excepting sometimes in the miliary papular and papulopustular eruption,
and then only, as a rule, in negroes. In this latter class, however, itch
ing, usually slight in character, is often complained of in the various
syphilodermata, especially the small lesional varieties named. The
limited papulotubercular and tuberculopustular area or areas of late
syphilis occasionally present a rough resemblance, especially upon the
scalp, but the distinct infiltrate, the copper or cut-ham color, the sluggish
character, the segmental and circinate arrangement, and usually evi
dences of destructive action, as shown by ulceration and scarring, atrophy,
and pigmentation, and the absence of itching are quite characteristic of
syphilis and wanting in eczema; moreover, the history and the clinical
behavior of the two affections are different.
296
INFLAMMATIONS
Squamous eczema of the palms and squamous syphiloderm of this
region at times resemble each other closely, but the former is more
apt to be diffused and often shows equal involvement with the fingers,
and in the latter regions occasional vesiculation, usually deep seated;
palmar syphiloderm is generally patchy, rather sharply defined, generally
wavy or segmental in outline, and often with a distinct circumscribed
infiltrate. Fissuring is not, as a rule, a marked feature of syphilis, while
it is frequently a pronounced feature in eczema; the syphiloderm is always
dry; eczema is noted at times to be moist, although this, in the palmar
region, is often entirely wanting throughout; in syphilis the eruption is
sometimes limited to the one hand: in eczema it is generally in both;
palmar syphiloderm is sometimes associated with a similar condition on
the soles: eczema rarely. Intense itching would indicate eczema, but
comparative lack of it has but little import, inasmuch as in squamous
eczema of this region it is occasionally trifling—not complained of,
and even denied; entire absence of itching, however, usually means
syphilis. Often a history of the latter disease is obtainable. It must
be admitted that in exceptionable instances the diagnosis as between these
two conditions is difficult, and the course of the disease under treatment is
to be noted.
Urticaria.—The ordinary wheals of urticaria will almost invariably
serve to distinguish it from eczema, in which such lesions are not observed.
Papular urticaria (lichen urticatus), in which, especially in young chil
dren, the lesions are small and often excoriated, resembles papular eczema
very closely, but in the former they are usually scattered and discrete,
whereas those of eczema are commonly on one or two regions, and often
show aggregation or solid patches. The papules of urticaria frequently
are noted to be left from pre-existing more or less typical wheals, and not
infrequently characteristic wheals, or the history of such, appearing from
time to time will aid in the differentiation.
There are some other diseases with which eczema may, if hurriedly
examined, be confused, but they are so exceedingly rare, even in the ex
perience of dermatologists, that special differentiation is scarcely called
for. These are prurigo, pityriasis rubra pilaris, pemphigus foliaceus, der
matitis repens, and Paget‘s disease, but they differ materially in appear
ance, behavior, and course, as the description of those several diseases
will show, and under several of which reference will be made to the more
important differential points.
Prognosis.—While eczema must, in the larger number of cases,
be considered obstinate, yet instances are relatively few in which relief
and cure cannot be effected, if proper opportunity is given to reach that
end; but this does not necessarily always mean permanency and freedom
from future attacks, unless the etiologic factors can be permanently re
moved or kept in abeyance, for if these come again into play, a recurrence
is possible, or, in many cases, even probable, the same as is observed in
almost all other diseases under the same circumstances. Eczema never
produces tissue destruction and never leaves scars or any other trace ex
cept on the legs, where, if of long duration, and especially in older people
ECZEMA
297
and those with varicose veins, some pigmentation may remain. Nor
has eczema any direct action upon the general health, but in severe, long-
continued, intensely itchy cases, from the consequent worry and loss of
sleep, the patient may become debilitated and neurasthenic. The prog
nosis in the individual case depends upon several factors—the locality
and extent of the disease, its duration and previous behavior, the remova
bility of the predisposing and exciting causes, the general health, and the
attention the patient can or will give to carrying out the treatment. It
may be said that acute or sudden attacks yield, as a rule, more readily than
those that are developed slowly and insidiously. The moist types are
generally also more responsive than the dry forms. Cases in which there
is a marked tendency to fissuring are usually obstinate.
Wherever the disease is situated, whatever its type, extent, and dura
tion may be, and whatever the age of the patient, its cure is never attended
with evil consequences, nor can its cure be, for the comfort and well-be
ing of the patient, too rapid. The few isolated instances among the hun
dreds of thousands of eczema cases in which an untoward result has been
reported (Brocq, Gaucher, Brooke, Duhring, Hallopeau and Leredde)1
as possibly due to rapid disappearance or suppression of the cutaneous
disease can be more reasonably, I believe, placed to the score of pure coin
cidence. Indeed, instead of such suppression being the cause, it is itself
probably the result, of the intercurrent constitutional disease, as it is a
matter of not uncommon observation that inflammatory skin affec
tions tend to subside temporarily upon the advent. and during the
course of a severe, especially febrile disease. In fact, one can safely say
that the secret of the attainment of a rapid suppression of an eczema
has yet to be learned, for, unfortunately, the cure is in the vast majority
of cases accomplished only after at least several weeks or months of per
sistent effort.
Eczema of the scalp often responds rapidly if the infiltration is not
very pronounced. As a rule, the hair suffers but little; in infants, from
the constant rubbing of the back of the head against the pillow, the hair
is sometimes rubbed off to a variable extent, but not permanently. On
the face, the disease is frequently obstinate, and especially in those whose
vocation subjects them to exposure to cold winds and dampness, or to
intense heat or to irritating substances. Eczema of the nares and of the
lips is somewhat variable as to the time and effort required, some cases
yielding readily. Eczema of the hands is often obstinate, occurring as it
does most frequently in those of the laboring classes, whose work in itself
may be the exciting cause, and which prevents a response to therapeutic
measures; in such cases, indeed, unless the occupation can be temporarily
suspended, a cure is usually impossible; and in many of these instances
resumption of the same work will often induce another attack. Eczema
of the nails is, as a rule, obstinate. Eczema of the crurogenital and anal
regions is also frequently rebellious, the friction, heat, and moisture of the
1 Brocq, Jour, de médicine de Paris, 1889, pp. 680 and 691, and Brit. Jour. Derm..,
1889, p. 105; Gaucher, Congrès Internat. de Derm, et de Syph., 1889, Compt.-Rend.,
p. 538 (refers especially to children); Brooke, Medical Chronicle (Manchester), 1889-90,
vol. xi, p. 206; Duhring, Cutaneous Medicine, part ii, p. 341; Hallopeau et Leredde,
Traité pratique de Dermatologie, Paris, 1900, p. 357.
298 INFLAMMATIONS
parts serving to keep up the disease or rendering the applications less
efficacious; the same may be said, but less strongly, of the disease in other
flexures. On the legs the malady, though severe, commonly yields more
or less readily, but occurring in those of advancing years, whose necessi
ties require them to be upon their feet many hours of the day, it is some
times slow to respond, and occasionally treatment fails absolutely until
this predisposing cause is lessened or temporarily suspended. In eczema
of the trunk the disease is rarely obstinate; about the nipple and the
umbilicus, however, it is often persistent. In acute, more or less general
ized eczema it responds, as a rule, somewhat rapidly, but after a certain
point is reached the progress is much slower, and in occasional cases the
disease persists upon one or two regions, most commonly the legs, for
some time after it has been removed from other parts.
Infantile eczema, as a rule, is, more especially if of the face and scalp,
its most common situations, quite amenable to treatment, though often
slowly so; if in the first year or two of life, in some cases slight recurrences
may be expected, but if the patient is aged four to five, the time when such
eczemas tend to get well spontaneously, not only will the disease often
respond surprisingly well, and to even treatment of an indifferent kind,
if not irritating, but the cure usually remains permanent. On other
parts the results are finally satisfactory also, but are not so quickly
obtained.
Treatment.—The earlier French teaching that eczema was due
to a diathesis, and that treatment was to be chiefly constitutional, and
the antithesis in the leading Vienna belief of about the same and later
period that the disease was essentially external in character, and required,
as a rule, external treatment alone for its removal, have gradually been
approaching a middle ground, which English and American physicians
have, upon the whole, for a long time maintained—that most cases, for
success or any permanency, demand both constitutional and local reme
dies. This, I believe, experience proves to be the rational view. It is
true many cases, some of which—as, for example, trade eczemas—seem to
be entirely local in their nature; and in such cases external treatment
alone will have satisfactory results. But even in some of these patients
underlying or concomitant systemic disorders often impede the progress
toward recovery, and if present should be given attention.
Constitutional Treatment.—This does not necessarily always mean
medicinal, for often attention to diet and other hygienic considerations
are more potent than drugs. While it is not possible to say that certain
foods directly induce eczematous conditions, still there are many, through
their difficult digestibility or through their influence upon the digestive
process, and possibly their absorption before thoroughly in condition for
such, which are often factors of some moment. For this reason the diet
in eczema cases should always be plain but nutritious, the meals taken at
regular times, and in sufficient, but not superfluous quantity. Such
foods as pork, in any form, salted meats, pastries of all kinds, veal, lob
sters, crabs, “gamy” fowls, fried dishes, gravies, sauces, cheese, pickles,
condiments, fruits, and like articles are to be avoided. Fish in some of the
cases is a questionable food, probably due to the fact that much of it on
ECZEMA
299
the market at the present day is from “cold storage,'’ and may have under
gone change. Oysters in the cold season are permissible, for they are
then usually well kept, but in warm, sultry weather they undergo rapid
deterioration and seem to develop intestinal toxins, and often aggravate
the disease. Excessive tea- or coffee-drinking is to be interdicted; like
wise indulgence in beer, wine, and other alcoholic stimulants; the malted
liquors especially seem to exert an unfavorable effect. Alcohol tends to
produce dilatation of the cutaneous vessels, besides, its influence in invok
ing or emphasizing defective kidney elimination, and is, therefore, even
in moderate quantities, especially damaging. To the very old and feeble,
accustomed to whisky or brandy, and who apparently need its support,
its continued use in moderate quantity should ordinarily be allowed.
The excessive use of tobacco should also be prohibited.
An ample dietary is to be found with the meats, beef, mutton, lamb,
poultry, and with the ordinary vegetables; potatoes should be taken in
moderation. In gouty and rheumatic cases an excessive meat diet should
be avoided, but there are some instances of these underlying states that
are due rather to the faulty starch digestion than to the meats, usually
in those in whom there is distinct digestive weakness, and such patients
will often do better with a fairly full meat allowance, together with the
less starchy vegetables. In troublesome cases, if of any extent, a rigor
ous milk diet with an allowance of meat or eggs once daily will sometimes
start the change toward recovery. In the matter of food, individual
idiosyncrasies should be considered. In fact, in obstinate and persistent
cases a purely meat diet had proved of curative aid in some instances
(Squire, McCall Anderson). The same experience has also been noted
with a purely vegetable diet (Neusser, Jarisch); the general condition of
the patient and his constitutional traits influencing the selection. An
other factor, not medicinal, and often of service, is the free drinking of
water, not during the meals, but between times; a full glass of water a
half hour to an hour before each meal, and at other times is often of serv
ice in promoting proper elimination through the kidneys. In some
patients the water before meals can be taken with greater advantage
quite hot. It is the free water-drinking, I believe, along with the regula
tion of the diet and the ordered exercise, and consequent regular bowel
movement, which is the strong element at the different mineral spring
resorts, the medicinal ingredients of the water scarcely being in sufficient
quantity to be of direct service. Systematic exercise, preferably in the
open air, moderate indulgence in calisthenics, living in well sun-lighted
rooms, and being as much as possible out-of-doors under the direct in
fluence of the sun‘s rays, are matters of great value in cases of any extent.
The value of light, and especially sunlight, as a therapeutic agent, is not,
I believe, as yet given the appreciation it deserves.
The plan of constitutional medicinal treatment, when such is indi
cated, as it usually is, is to be based upon the indications in the indi
vidual case. A careful examination into the patient‘s general health
will usually give the cue to the line of treatment to be adopted. There
are no specifics for this disease; arsenic, which was formerly in great
vogue, is now known to be only occasionally of service, although it is
3oo
INFLAMMATIONS
still greatly used, often to the patient's disadvantage, by the general
profession. It should, as a rule, be the last remedy resorted to, rather
than the first, as other plans are much more generally successful. This
remedy will be referred to again. The aim in all cases is to see that the
important emunctories of the body—the intestinal tract and the kidneys
—are performing their work; sometimes this is accomplished by attention
to hygienic means alone, as already indicated, but often it needs medicinal
re-enforcement. A proper action, and preferably free action, of the bowels
is a most essential desideratum in the management of eczema.
In some cases the constitutional treatment, or, properly speaking,
management, need not go beyond the measures just indicated; but
in many instances, as noted in discussing etiology, there is disturb
ance of the digestive apparatus, of which constipation is but a feature.
In many of these patients the daily or occasional administration of a
laxative, along with an ordinary tonic digestive mixture, associated
with mild soothing or slightly stimulating external applications, will
soon bring about recovery. As a rule, the various salines, such as
Epsom salts, Rochelle salts, sodium phosphate, and the saline aperi
ent mineral waters, are of most service in eczema cases. A frequently
used and valuable saline laxative tonic is that known as “mistura ferri
acida,” the formula for which is as follows:
R. Magnesii sulphat., 3j-iss (32.-48.);
Ferri sulphat., gr. iv (0.265);
Ac. sulph. dilut., f3j (4.);
Aquæ menth. pip., q. s. ad f3iv (128.).
Sig.—A tablespoonful in a full tumblerful of water about twenty minutes before
breakfast.
If not sufficiently active, the dose may be increased somewhat, or a
smaller amount can be taken before each meal. In gouty or rheu
matic cases the acid should be omitted. Another saline mixture of
value, and which can be used as a substitute for Carlsbad salts, and
which is in reality more efficient for these cases, is: R. Granulated sodium
sulphate, 3x (40.); sodium bicarbonate, 3iv (16.); sodium chlorid, 3ij
(8.); the dose is from one to two teaspoonfuls in a tumblerful of water
twenty to thirty minutes before breakfast, or in smaller dosage before
each meal. It is to be kept in a closely stoppered, wide-mouthed bottle,
as it is hygroscopic Patients who do not seem to bear salines well can
take the following bitter laxative tonic, and which can be given in many
cases to advantage: R. Sodii salicylat., 3j-ij (4.-8.); ext. cascaræ
sagradæ fl., f3j-iv (4.-16.); tinct. nucis vomicæ, f3ij-iv (8.-16.); and
tinct. cardamom comp., or tinct. gentian comp., q. s. ad f3iij (96.); of this,
a teaspoonful in water after each meal. The quantity of cascara should be
increased or diminished according to the effects; ordinarily, two to three
drams (8.-12.) in such a mixture will be required. In some cases, espe
cially if there is torpid liver action, an occasional laxative dose of calomel,
usually 1 to 3 grains two or three times weekly, will not only be a satisfac
tory laxative, which can be taken for a time, but will sometimes exert a
favorable influence upon the disease. Or, instead of taking it in this
dosage, the small triturate of 1/10 of a grain (0.0065) of calomel and 1 or 2
ECZEMA
30I
grains (0.065-0.13) of sodium bicarbonate can be given at half or hour
intervals until laxative effect is brought on—not more than 10 to 15
tablets, and repeated every few days. Among other satisfactory laxa
tives to which recourse may be had are the aloin-strychnin-belladonna
pills, the compound licorice powder, and the plain fluid extract of cascara
sagrada.
In some of the eczema cases in which stomachic acidity is a factor
sodium bicarbonate, or if there is fermentative tendency, sodium ben-
zoate, 5 to 10 grains (0.33-0.66) three times daily, alone or often associated
with advantage with a bitter, will prove of benefit. In other cases
hydrochloric acid often acts satisfactorily; as a rule, however, acids are not
so desirable in eczema as alkalies. In many instances of digestive debility
the various digestive aids, such as pepsin and pancreatin, can be given
along with a bitter stomachic In some of these cases, usually those of
stomachic and intestinal indigestion or catarrh, in which diarrheic attacks
come on from time to time, laxatives must be used with care; in such
patients or at such times bismuth, charcoal, and salol can be administered.
In short, in these cases the aim is to remove any existing dyspeptic con
ditions, to improve the digestive tone, and to meet any special indications
as they may arise. In persistent stomachic catarrh occasional lavage of
this organ is to be tried.
In another class of patients—the neurasthenic class—invigorating
measures of all kinds are to be advised; in some, absolute or relative
rest; in others, daily calisthenics and outdoor exercise; general massage
in suitable cases; and the use of such drug tonics as strychnin, quinin,
the hypophosphites, cod-liver oil, and arsenic. It is in this class, and
especially when the eruption is extensive, that electricity, in the method
of general galvanization, seems to be of service; running a strong current
down the spine is also of value. It is probably more particularly in
neurotic cases that counterirritation (Crocker)1 by means of mustard
plasters, heat, friction, or wire-brush electrode (Hyde)2 over the corre
sponding vasomotor centers occasionally proves of value. It is not ad
visable, however, in my judgment, to use such counterirritants in instances
in which there is still tendency to outcropping of new areas. Duhring com
mends antipyrin and, bromids in moderate doses for neurasthenic cases.
In other cases—the gouty and rheumatic—the salicylates, salol,
salophen, salicin, sodium bicarbonate, potassium bicarbonate, potas
sium acetate, the salts of lithium, and exceptionally colchicum, are the
most important remedies, along with attention to diet in the lines already
indicated. In another class of cases the disease seems to be kept up by a
general debilitated state of the system, and in these there is nothing so
valuable, if it can be taken and digested, as cod-liver oil. The dose should
not be large—from ½ to 2 fluidrams (2.-8.) will be sufficient; in fact, for
its good effects the dose of a dram (4.) need rarely be exceeded, and when
so limited, there is less chance of disturbing digestion, and thus necessi
tate the discarding of a valuable remedy. With this may be administered
fairly large doses of strychnin, and in some cases small doses of iron.
1 Crocker, Brit. Med. Jour., July 9, 1887, p. 66.
2 Hyde, “Diseases of the Skin,” Twentieth Century Practice, vol. v, p. 196.
302
INFLAMMATIONS
There are other classes of patients, etiologically considered, but
the several named comprise most of the cases. For instance, mala
ria, diabetes, and albuminuria may at times be considered active un
derlying conditions, and then proper treatment of these will aid materi
ally in rendering the external treatment more effective. In some in
stances, however, it is difficult to assign a cause for the disease, either
constitutional or external. Under such circumstances the treatment is
entirely empirical, being chiefly conducted on the assumption that an
obscure underlying gouty cause is operative, or some slight or un
recognizable assimilative or digestive irregularity. If treatment upon
such lines seems futile, there are certain special remedies, variously
indorsed, that may be tried experimentally.
Arsenic has long been extolled as having a specific influence in ec
zema, but it may be safely stated that it is prescribed by specialists for
alleged specific effect in only a small percentage of cases. It is often
given in small doses as a tonic along with other drugs of the same class,
and is especially valuable in patients with underlying anemia, chlorosis,
etc. (Hardaway, Morrow, Jarisch, and many others). It may be tried,
however, in obscure cases for its specific effect. The drug is a cutaneous
stimulant, and should not, therefore, be employed in acutely developing
cases, nor, as a rule, in those of an acute type, as aggravation will almost
certainly follow. Its special field is thought to include those of a sluggish,
papular, or squamous type, and in some such instances I have occasionally
seen it act most happily, but even in especially indicated cases it often
fails to make an impression, and sometimes is detrimental. It should be
continued for some weeks unless the disease seems aggravated or the
drug causes positive systemic disturbance, usually digestive or neu
rotic in character. Among other remedies variously extolled may be
mentioned viola tricolor (Piffard,1 Ferguson), oil of copaiba, oil of
turpentine (Crocker), tar (McCall Anderson, Duhring), jaborandi or
pilocarpin (Simon, Jamieson), ergotin (Lewin, Jarisch), ichthyol (Unna),
and wine of antimony or tartrate of antimony (Morris, Jamieson2).
Eczema in infants and young children is most frequently attribu
table to improper feeding, to digestive irregularities, and to constitu
tional debility. Special attention must, of course, be given to the
feeding, and it is to be remembered that in artificially fed infants milk,
sterilized or pancreatinized, is to constitute the chief and, as a rule,
the only food. Not much is to be hoped for permanently in these
cases of eczema in infants and children unless the dietary is rigorously
supervised. Lime-water added to the milk, a tablespoonful (16.)
to the 4 ounces (128.), is sometimes a help. Constipation is to be cor
rected by the administration of fluidextract of cascara sagrada, gray
powder, or castor oil. Of the first, the dose is from 2 to 10 drops (0.133-
0-65), given in a little syrup of ginger or orange or other flavoring excipi-
ent; the dose of gray powder is from 1 to 2 grains (0.065-0.13) at bed-
1 Piffard, “On Viola Tricolor and Its Use in Eczema,” Med. Record, April 29, 1882;
Ferguson, “Viola Tricolor in Chronic Eczema,” Canadian Jour. Med. Sci., April, 1882.
2 Malcolm Morris, Brit. Med. Jour., Sept. 22, 1883, P- 572; Jamieson, Brit. Jour.
Derm., 1891, p. 271.
ECZEMA
303
time every second or third night; castor oil may be given with an equal
part of the spiced syrup of rhubarb, in the dose of from one-half to a
teaspoonful at bedtime, or three times daily, depending upon the age of
the child and the effect produced. Enemata and glycerin suppositories
may also be resorted to from time to time. In these little patients a small
dose of sodium bicarbonate three times daily will sometimes influence
the disease favorably. In fact, in these cases the digestion must be
looked after carefully. In many of these infants the nutrition is below
the standard, or the patients are of the so-called strumous diathesis.
Under such circumstances cod-liver oil is a most admirable remedy, given
in emulsion with calcium lactophosphate, or in mixture with an equal
part of lime-water; of either of these the dose is from one-half to a
teaspoonful three times daily. A mixture which I have often found use
ful in such cases and in which constipation is present is one composed of
cod-liver oil and castor oil in variable proportion, according to the bowel
torpidity, and with several drams of spiced syrup of rhubarb to the 3
ounces (96.), to give it flavor. In infantile eczema cases the possibility
of the disease being dependent upon or aggravated by reflex irritation is
to be borne in mind; the question of an adherent prepuce, an emerging
tooth, or intestinal parasites should receive attention.
External Treatment.—The external treatment of eczema is of essen
tial importance, and must be resorted to in every instance. In certain
cases, as already remarked, external applications alone suffice to bring
about a cure. There are certain general principles in the local manage
ment of this malady that should be kept well in mind. The affected
surface is to be freed from the products of the disease—the crusting and
the scaliness. This is best accomplished by means of oily or unctuous
applications, supplemented, in suitable cases, from time to time, with
washing with soap and warm water. In acute cases, however, and also,
as a rule, in those of an acute type, soap and water are rarely admissible;
in such instances cleansing can usually be effected by gently wiping
with cold cream or petrolatum. Many cases in which there is but a
slight degree of scaliness or crusting the remedial treatment alone, es
pecially if consisting in the application of ointments or oils, will serve in
itself to remove such products. In those of more marked scaliness or
crusting, plain carbolized oil (gr. v-f3—0.33-32.) or liquid petrolatum
may be used freely, applying it every hour, or flannel cloths soaked
in oil can be applied and allowed to remain in contact with the affected
surface; after several hours or half a day the parts are then washed with
warm water and a mild toilet soap. Or the remedial application may even
in such instances in the very beginning be supplemented with the daily
washing with soap and water, and as soon as the surface is freed, the latter
can be omitted or used at intervals. If the crusting is abundant and ad
herent, a plain poultice or starch poultice, and preferably made with 2
per cent, boric acid solution, may be used instead of oily applications
for the purpose of softening, and be followed by the soap-and-water
washing.
After removal of the scaliness or crusting, soap and water are, as
a rule, to be used as infrequently as possible in average cases of the acute
304
INFLAMMATIONS
and subacute types of the disease, as both are irritating in their effect;
in instances of marked irritability, or aggravation from such, the parts
can be cleansed from time to time with cold cream, vaselin, or almond oil.
In certain cases, however, more especially those of chronic sluggish
character, the use of soap and water has a therapeutic value.
The selection of the plan of medication and the strength and char
acter of the applications depend chiefly upon the type of inflammatory
action. Even in long-continued cases of the disease the type of inflam
mation is at times persistently acute, although more frequently subacute.
On the other hand, some are from the outset sluggish or chronic in charac
ter. For a proper conception of the management of eczema, therefore,
the degree of inflammatory activity must be considered; it matters not
upon what part of the body the disease may be located. In great measure,
too, upon the character and type depends the choice of whether lotions,
dusting-powders, ointments, oils, or fixed dressings shall be employed.
This will be indicated as the various inflammatory grades are considered,
but there is no absolute rule. It can, however, upon the whole, be said
that lotions with sediments are most useful in the acute and subacute
moist types; that clear lotions may be used in such instances, as also
in dry types, often with benefit, if \ to 2 drams (2.-8.) of glycerin are
added to the pint (500.), but, as a rule, more satisfactorily when conjointly
with ointments; clear lotions can also be used in erythematous types, some
times alone, but usually preferably with a supplementary dusting-powder.
In thickened, subacute and sluggish cases ointments and fixed dressings
(gelatin, etc.) are generally most useful, and especially in the dry forms.
Oils are also of value in the latter, but their use is limited.
A substitution of one plan or form of application for another is
often necessary, either for the reason that no improvement had followed
or in consequence of change of type—from moist to dry—as the result
of the treatment first employed. Nor is it always possible to say that a
given remedy will be of service, some skins exhibiting marked idiosyn
crasy; all changes should be instituted cautiously, and, as a rule, the ap
plication tried on a limited area first. It should, moreover, be a dermato-
logic axiom, and most applicable in eczema, that so long as a selected
remedy or plan is benefiting it should be continued.
The methods of applying the remedies are of importance. The
clear washes can be simply applied with a soft linen rag or a pledget
of absorbent cotton or with an atomizer; those containing sediments
dabbed on for several minutes and allowed to dry on, or pieces of linen
cloths can be kept constantly applied and freely wet with it from time
to time. Lotions are not to be rubbed on. Oily, emulsion-like applica
tions can be applied in the same manner as the sediment lotions. In
sluggish cases plain oily applications can be rubbed in, and usually with
considerable vigor. Ointments are applied in all types of a moist char
acter, and also in the acute dry type, either by anointing or spread upon
lint. The latter is more efficient, but not always practicable. In dry,
sluggish, subacute and chronic types they can be rubbed in, using a vari
able amount of friction, and if increased action is desired, can then be
applied as a spread plaster. If at any time the sediment of lotions or the
ECZEMA
305
pastes should mass upon the surface and adhere firmly, softening with an
oil or cold cream or vaselin will usually suffice for removal.
One of the most troublesome phases of the management of eczema
cases is the control of the itching, and often attention must be given,
for a time at least, to this point exclusively. Ordinarily the plans of
treatment to be considered will hold this symptom within bounds, but
occasionally the selected plan must give way to another, or recourse must
be had to the special remedies useful in this condition. The addition of
carbolic acid, thymol, or hydrocyanic acid to the selected application will
usually suffice; in exceptional instances, if relief is not afforded, applica
tions of hot water as hot as can be borne, and more certainly if it contains
½ to 1 grain (0.033-0.065) of sodium bicarbonate to the ounce (32.), will
bridge over the pruritic attack. To the pint of lotion carbolic acid can be
used in the quantity of ½ to 2 drams (2.-8.); thymol, 8 to 16 grains (0.5-1.);
dilute hydrocyanic acid, 1 to 4 drams (4.-16.); and to the ounce of oint
ment carbolic acid, 2 to 30 grains (0.133-2.); thymol, 1 to 10 grains
(0.065-0.65); dilute hydrocyanic acid, 5 to 20 minims (0.35-1.35).
Menthol can also be used in ointment, 1 to 10 grains (0.065-0.65) to the
ounce (32.). Of these, carbolic acid is the most valuable. Thymol,
in lotion, needs some alcohol and glycerin for its solution.
Unless one is especially skilled in the management of diseases of
the skin it is a good plan to begin the treatment of all cases, even though
somewhat sluggishly inflammatory, with the remedial applications to
be mentioned as appropriate for the acute type; much can frequently be
accomplished, and at least the patient‘s confidence is gained, and then
one can, if it seems necessary, go ahead more boldly.
In acute or actively inflammatory cases of any variety, and in almost
all cases in which there is scarcely perceptible infiltration and no epidermic
thickening, mild applications alone are well borne. In such the conjoint
use of a boric acid lotion, 15 grains (1.) to the ounce (32.), and a mild
ointment, such as the zinc oxid, cold cream, or petrolatum, will often
give relief; the zinc ointment is probably the most satisfactory. The
same may be said of the treatment (White) with lotio nigra, pure or pref
erably with an equal part of lime-water, in conjunction with such an
ointment; if over a large surface, the dilution with lime-water should be
greater, to avoid the possibility of mercurial absorption. The lotion is
first thoroughly dabbed on for several minutes or longer, and allowed to
dry or partly dry; then a small quantity of the selected ointment is
gently smeared over; or the ointment may be applied spread upon lint
or linen. If the disease is extensive and there is danger of chilling, the
surface can be merely moistened with the selected lotion, and then the
salve applied immediately; or preferably a small part may be thoroughly
gone over at a time, and as soon as anointed another part treated. When
the application is repeated, which should be done every several hours,
or, at the least, two or three times daily, the parts are first gently wiped
off with a piece of soft linen or absorbent cotton; in many of the cases
in which the ointment was merely smeared on it has entirely disappeared
by the time another application is to be made. I cannot speak too highly
of these two plans, nor urge too strongly their value and safety in the be-
20
306
INFLAMMATIONS
ginning management of most cases; it is only in extremely rare instances
that either proves irritating. The boric acid lotion is especially valuable,
probably by its mild antiseptic property,1 and is, in my practice, almost
indispensable. The use of a compound lotion alone is often beneficial
in the erythematous and papular varieties:
R. Acid, borici, 3ij (8.);
Acid, carbolici, 3ss (2.);
Glycerini, mx-xxx (0.65-2.);
Aquæ, q. s. ad Oss (250.).
This can be used with or without an ointment. Its effect is some
times enhanced by applying, immediately after it dries, a simple or com
pound dusting-powder, such as named below. An oily lotion or lini
ment, soothing in these acute cases, is one composed of equal parts of
lime-water and sweet almond oil, with ½ to 2 grains (0.033-0.13) of
carbolic acid or resorcin to the ounce (32.). Or in these same types and
also in the vesicular form of the disease the following calamin-and-zinc-
oxid lotion may be used:
R. Calaminæ,
Zinci oxidi ââ 3ij-iv (8.-16.);
Liquor, calcis, f3ij (64.);
Aquæ, q. s. ad Oss (250.).
This is to be dabbed on freely several times daily; it will act more satis
factorily if linen cloths kept wet with it are constantly applied. If the
itching is troublesome, to the last lotion may also be added from 15 grains
to 1 dram (1.-4.) of carbolic acid, or from 2 to 8 grains (0.13-0.53) of
thymol, or from 8 grains to ½ dram (0.52-2.) of resorcin, to 8 ounces (250.).
These several last-named drugs may be used alone as lotions, in the
strengths indicated, especially in the erythematous and papular varieties.
Another mild soothing lotion of benefit in cases of acute type consists of:
R. Zinci oxidi, 3ij-iv (8.-16.);
Acid, carbolici, gr. xx (1.3);
Mucilag. acaciæ, f3ij (7-5);
Emuls. amygdalae, f3ij (60.);
Aquæ, q. s. ad f3viij (250.).
Liquor carbonis detergens,2 from 1 to 2 drams (4.-8.) to the pint (500.)
of water, or in the same proportion added to the several lotions named,
1 See suggestive paper by Klotz, “The Principles of Antisepsis in the Treatment of
Eczema,” Jour. Cutan. Dis., 1894, p. 99. Only the milder antiseptics are permissible
in eczema, the employment of the stronger surgical antiseptics, such as corrosive
sublimate solutions, formalin, strong carbolic-acid solutions, etc, are usually aggra
vating.
2 Liquor carbonis detergens is a proprietary coal-tar preparation made by Wright &
Co., London; it is essentially a solution of coal tar in soap-bark tincture. Equally
as good, however, and even superior, is one which I can strongly commend, used for
many years at the Skin Dispensaries of the University of Pennsylvania, Jefferson
Medical College Hospital, Philadelphia Dispensary for Skin Diseases, and Howard
Hospital, made as follows: Coal-tar, 4 parts; strong soap-bark tincture, 9 parts; digest
for eight days, frequently shaking and stirring, and finally filtering. The soap-bark
tincture is made with 1 pound soap-bark to 1 gallon 95 per cent, alcohol, digesting for a
week or so. More recently Professor Duhring, Amer. Jour. Med. Sci., May, 1894, has
modified this formula, using 1 part coal-tar to 6 parts soap-bark tincture, and suggested
ECZEMA 307
is useful in these cases. Ichthyol as a lotion, from 1 to 4 drams (4.-16.)
to the pint (500.), also proves of service. Lead-water (liquor plumbi
subacetat. dilut.) with several or more parts water is likewise a soothing
application, sometimes beneficial in the acute types.
With the lotions free from sediments their use with supplementary
applications of a dusting-powder after the lotion has dried on, or before
completely dry, is often an admirable method, especially in the erythem-
atous and papular types.
Powders are, indeed, frequently used alone in the first few days, in
extensive erythematous acute cases of this class, and sometimes give
a good deal of relief, and are more especially serviceable when the affec
tion occurs in regions where two surfaces come in contact. They are also
occasionally used in the secondary stages of the more acute vesicular
disease, for their desiccating influence, especially in cases in which oint
ment applications and lotions are found to be irritating. The powders
most commonly employed are zinc oxid, talc, boric acid, lycopodium,
starch, magnesium carbonate, rice-flour, zinc oleate, zinc stearate, and
bismuth subnitrate. The following is a serviceable and clean combina
tion: R. Pulv. ac. borici, gr. xxx (2.); talci, zinci oxidi, âá 3ss (16.).
As a rule, however, it will be found that the conjoint use of a lotion and
powder is preferable to the latter alone.
In some cases of the acute inflammatory type ointments are found
more comforting, although in the early stages, as a rule, not so fre
quently so as lotions. They are more especially useful in the dry vari
eties, and when there is a tendency to desquamation and cracking.
Even in most of these instances the preliminary application of a lotion,
more particularly the boric acid lotion, seems to be an advantage.
Zinc oxid ointment, already referred to, can be used alone, and is ex
tremely valuable, often affording relief; if the parts feel tense and hot,
an ointment made of this and an equal part of cold cream can take its
place; instead of the zinc oxid constituent, bismuth subnitrate can be at
times substituted to advantage. Cold cream itself is,, indeed, a valuable
salve in these cases, and especially when used conjointly with a lotion.
In fact, cooling salves—those containing water—are usually most sooth
ing. For this reason an ointment (Unna) composed of lanolin 1 part,
lard, 2 parts, and rose-water 3 parts, can often be used as a soothing
refrigerant application; or in place of the rose-water lead-water or lime-
water can be substituted (Duhring) with advantage, especially in
markedly acute types, the latter ingredients adding to its soothing prop
erties. Diachylon ointment, if well and freshly prepared, is also sooth
ing and mildly astringent, but it is difficult to get a good preparation;
in the latter event, or if not fresh, irritation often follows its application.
Plain petrolatum suits some cases, but disagrees with others, and, as a
rule, is not to be used alone in the acute type, but as a base or part constit-
the name compound tincture of coal-tar (tinct. picis mineralis comp.); it is, however,
weaker than the other formula named. Many other formulas are to be found in litera
ture, some good, some indifferent, and some bad. The recent papers by Brocq (“Le
Goudron de Houille Brut en Dermatologie,” Annales, 1909, p. 1, with brief review and
some references) and by Dind (“L‘emploi du Goudron de Houille (coaltar) dans les
applications cutanées,” ibid., p. 170) give various formulas and combinations.
308 INFLAMMATIONS
uent of a base for incorporation of powdery ingredients it is often per
missible and satisfactory. The following I have often used in these cases
with benefit:
R. Calaminæ,
Zinci oxidi, ââ gr. xl (2.65);
Amyli, 3j (4.) ;
Ac. salicylici, gr. iij-x (0.2-0.65);
Petrolati, q. s. ad 3j (32.).
One composed of calamin, 3j (4.), and ungt. zinci oxidi, 3vij (28.),
is also often valuable. In pustular eczema of the acute type lotions
and ointments conjointly used afford the most satisfactory results, and
a minute quantity of white precipitate, 1 to 3 grains (0.065-0.2) to the
ounce (32.) of ointment, will add to the favorable effects in some in
stances. Boric acid ointment is also useful in such cases.
Very often, when salves, such as described, will not agree, the so-
called pastes (Lassar, Unna, Gründler)1 can be employed. In fact,
these latter are often the more acceptable, and act satisfactorily. They
possess a certain porosity, and while they are protective, they do not
entirely block up exudation. The salve mentioned above, containing
zinc oxid, calamin, and starch, is somewhat of this nature. The type
of this class, is, however, the following (Lassar‘s paste):
R. Zinci oxidi,
Amyli, ââ 3ij (8.);
Petrolati, 3iv (16.).
In this is commonly incorporated 3 to 10 grains (0.2-0.65) of salicylic
acid. The latter amount is usually added, and when so constituted
the paste is generally known as the “salicylic acid paste,“ “salicylated
paste.” In fact, when “Lassar‘s paste” is referred to, this salicylated
paste is usually meant. It is a most admirable preparation, not only
in the less actively acute types, but in the subacute cases. Another
paste which is also satisfactory is one similar to that given: R. Zinci
oxidi, amyli, ac. borici, ââ gr. lxxx (5.33); ac. salicylici, gr. iij-x (0.2-
0.65); petrolati, 3iv (16.). To these, and in fact to the salves already
mentioned, in extremely itchy cases, can be added to the ounce (32.)
1 to 3 grains (0.065-0.2) of carbolic acid; a stronger proportion—up to
10 grains (0.65)—is sometimes permissible, especially in the less actively
acute cases.
In eczema of a subacute or moderately inflammatory type, whether
beginning as such or evolving from the acutely inflammatory cases,
and in which there is distinct infiltration or epidermic thickening, it is
advisable to begin the treatment with one of the several applications
suggested for the acute type. Too much stress cannot be laid upon this
point, for often the quickest and most satisfactory results are thus
attained. Cautiously, if necessary, as it frequently will be, the various
1 Lassar, “Ueber Salicylpasten,” Monatshefte, 1883, vol. ii, p. 97; Unna, “Die
Pastenbehandlung der entzündlichen Hautkrankheiten, insbesondere des Ekzems,,,
ibid., 1884, vol. iii, p. 38; Gründler, “Ueber Pasten,” ibid., 1888, vol. vii, p. 1029; G. W.
Wende, “Ointments and Pastes,” Amcr. Med. Quarterly, June, 1899 (an excellent ex
position of the subject).
ECZEMA
309
active ingredients named in some of the lotions and ointments—as, for
instance, carbolic acid, salicylic acid, etc—can be added in greater pro
portion. A lotion containing ½ to 2 ounces (16.-64.) of liquor carbonis
detergens to the pint (500.) of water is extremely valuable in many cases,
and can be used plain as such, or this tar product can be added to any
of the several lotions already named. This is one of the most valuable
tar preparations in these cases, and least likely to disagree, but, as with
all tarry applications, it should be used cautiously at first, as some skins
are intolerant to this drug. The carbolized boric acid lotion referred to
may also be prescribed with from 2 to 5 grains (0.13-0.32) of tannic acid
to the ounce (32.). Resorcin is also valuable in this type, employed as a
lotion of from 3 to 10 grains (0.2-0.66) to the ounce (32.), or as an oint
ment of from 10 to 20 grains (0.65-1.33) to the ounce (32.). Ichthyol
in from a 2 to a 5 per cent, lotion is sometimes valuable. The following
is also useful:
R. Zinci oxidi, 3ij (8.);
Liquor, plumbi subacetatis diluti, f3vj (24.);
Glycerini, f3ij (8.);
Infus. picis liquidæ, q. s. ad f3iv (128.).
In limited areas, especially of a slightly moist type, painting on a satu
rated solution of picric acid (Maclennan, Thiéry, Leredde, Radaeli)
two or three times daily for three or four days, and then applying emol
lients, waiting until the film thus formed comes off, is sometimes of ser
vice. In these cases, as well as in those of a chronic type, an occasional
painting (every five to ten days) with a 1 to 10 per cent, aqueous solution
of silver nitrate, or with a 1 to 3 per cent, solution in sweet spirits of niter,
proves valuable, more especially in the slightly moist cases.1
In this type the results are usually better when a lotion, if employed,
is followed by a salve; and an occasional stirring up of the surface with
a strong lotion, followed by one of the soothing ointments, sometimes
constitutes a good plan. As a general rule, however, soothing remedies
are here, as in the acute type, to have first place. Some cases seem to
do better on ointments alone. White precipitate can be added to the
several already named, in the proportion of 5 to 30 grains (0.33-2.) to
the ounce (32.). Calomel, in the same proportion, acts well in many
instances, and is the one I most frequently have first recourse to when
stronger applications are found necessary:
R. Hydrargyri ammoniati seu hydrargyri
chloridi mitis, gr. v-xxx (0.32-2.);
Acidi carbolici, gr. v-x (0.33-0.65);
Ungt. zinci oxidi, 3j (32.).
If this last ointment is to be rubbed in, as in erythematous and squamous
areas, the zinc oxid ointment can sometimes be replaced with advantage
by petrolatum, lard, or cold cream. Another formula (Klotz2) that is
useful, especially as a preparatory measure, in subacute thickened eczema
1 See interesting paper by Dunn, “Nitrate of Silver in Dermatology,” Pennsylvania
Med. Jour., Jan., 1901.
2 Klotz, New York Med, Jour., Sept. 17, 1887.
310
INFLAMMATIONS
of the hands and extremities, for constant application in the form of a
plaster, consists of:
R. Acidi salicylici, gr. x-xx (0.65-1.33);
Emplastri plumbi, 3iiss (0.10);
Emplastri saponis, 3iiss (0.10);
Petrolati, 3iij (12.). M.
The same can be said of a 5 per cent, salicylated soap-plaster (Pick1).
An ointment of alumnol or of aristol, from ½ to 1 dram (2.-4.) to the
ounce (32.), and an ointment of acetanilid, from 5 grains to 1 dram
(0.33-4.) to the ounce (32.), prove beneficial in some instances. The
tarry ointments may be used in these cases, but they should be weak and
employed at first cautiously, as they may disagree. The following are
mild, and can be often prescribed with great advantage; the first one
is the milder and safer for beginning a change in the treatment, and one
that can be recommended:
R. Liquor, carbonis deterg., 3j_ ij (4.-8.);
Ungt. zinci oxidi, q. s. ad 3 j (32.). M.
Or
R. Ungt. picis liquidæ, 3j-ij (4-8.);
Ungt. zinci oxidi, q. s. ad 3 j (32.). M.
If the larger quantity of the liquor carbonis detergens is prescribed
in the former, the zinc oxid ointment should be partly replaced (about
5j-ij (4.-8.)) with powdered starch, simple cerate, or lanolin, otherwise
the resulting ointment would be too soft. The salicylic acid paste makes
a good base for it.
These cases may at times be satisfactorily treated with some of the
fixed dressings, especially the salve-mulls and gelatin applications, the
medication varying somewhat, usually being zinc oxid, ichthyol, boric
acid, small quantities of tar, or resorcin. The salve-mulls2 (Unna) are
especially valuable in irritable cases,—the zinc oxid and the boric acid
salve-mulls,—and can be used with safety, both in this type and the acute
type cases. They are kept constantly applied, changing once in the twelve
or twenty-four hours, according to circumstances. My experience has
chiefly been with the two named, although they are made with various
other medicaments incorporated.
The gelatin applications (Pick, Unna, Morrow, and others)3 are most
admirable and constitute a valuable method of treating many cases of
the disease, more particularly when upon the lower extremities. They
are especially useful in cases of this type of inflammatory action, but they
1 Pick, Verhandlungen der Deutschen dermal. Gesellschaft, I. Congress, Vienna,
1889.
2 The salve-mulls, and also the plaster-mulls to be referred to, are made by Beiers-
dorf, Germany, and imported, through Lehn and Fink, New York. They are some
what expensive, but have not yet been successfully imitated in this country.
3M. Pick, “Die therapeutischen Verwendung arzneihaltiger Gelatine bei Haut-
krankheiten,” Monatshefte, 1883, vol. ii, p. 33; and Prager med. Wochenschr. 1883, No.
6; Unna und Beiersdorf, “Leimglycerin als Konstituens in der Dermatotherapie—
Gelatinæ glycerinatæ medicatæ,” Monatshefte, 1883, vol. ii, p. 37; and Jour. Cutan.
Dis., 1884, vol. ii, p. 54 (this paper contains tables of formulas for various drugs with
gelatin, glycerin, and water, both for soft and hard preparations); Morrow, “An Im
proved Method in the Treatment of Certain Forms of Skin Affections,” Med. Record,
March 1, 1884; Eddowes, Medical Times and Hospital Gazette, Sept., 1899.
ECZEMA
311
can also be used in some of those of the more acute variety, and are like
wise of distinct service in the sluggish cases. There are various formulas
given, but the most generally useful are the following—hard preparation:
Gelatin, 4 parts; glycerin, 1 part; water, 8 parts (Morrow); soft prepara
tion—and that which I have used most frequently: gelatin, 2 parts;
zinc oxid, 1 part; glycerin, 3 parts; water, 4 to 6 parts, and to this prep
aration is added 2 per cent, of ichthyol, 1 per cent, of carbolic acid, or
salicylic acid. That containing zinc oxid and ichthyol is most service
able; the same ingredients can also be added to the first formula. When
needed for use, it is melted over a water-bath (a double farina or oat
meal boiler answers the purpose), and applied with a broad brush of
from 1 to 3 inches wide. If desired, if the harder preparation is used,
it can be allowed to dry on, and then simply dusted over with an indiffer
ent powder. I prefer using the softer gelatin preparation, and then
before the gelatin is dry to apply a thin gauze bandage; this adds to the
completeness and effectiveness of the dressing. This can ordinarily be
left on three to five days; when its removal is desired, it is softened thor
oughly with warm or hot water, after which it readily comes off; a fresh
dressing then is applied.
Linimentum exsiccans (Pick1), of which tragacanth is the basis, is
another dressing which dries on, but it is not comparable to the gelatin
application, although it can often be more conveniently used on some
situations than the latter. The following is the formula: R. Tragacanth
5 parts; glycerin, 2 parts; boiling water, to make 100 parts; to this is
usually added, to preserve it, 2 per cent, of boric acid. It can be variously
medicated, that with 5 to 10 per cent, of zinc oxid, and 0.5 to 1 per cent,
of carbolic acid, is most commonly used. This dries slowly, and I believe
is not so good as one with acacia as the base: R. Zinci oxid., 2 parts;
glycerin, 1 part; and mucilage of acacia, 5 to 8 parts; the various drugs
can also be added to this. Somewhat similar to that of Pick‘s, but su
perior, is one made with bassorin (Elliot2): Bassorin, 48 parts; dextrin, 25
parts; glycerin, 10 parts; and water to make 100 parts; it should be pre
pared cold. Zinc oxid, ichthyol, and other medicaments can be incor
porated. These several drying paints are, as a rule, not practicable in
hot weather, as the increased perspiration makes them sticky. After
the application dries on a powder can be dusted over.
In the management of eczema of chronic (sluggish) inflammatory
type in which there are moderate or pronounced infiltration and epidermic
thickening, the various applications already indicated in the treatment
of the acute and subacute types, especially of the latter, can be tried first.
In many of these cases, however, these will only bring about slight
betterment, and stronger methods must be resorted to. An occasional
or frequent, according to circumstances, vigorous shampooing with
sapo viridis, conjointly with the above lines of treatment, will often bring
about a favorable result. After the soap-washing the parts should, of
1 F. J. Pick, “Ueber die Anwendung eintrocknender Linimente (Linimenta exsic-
cantia) bei der Behandlung von der Hautkrankheiten,” Archiv, 1891, p. 633.
2 Elliot, “Bassorin Paste: A New Base for Dermatological Preparations,” Jour.
Cutan. Dis., 1891, p. 48; “Bassorin Paste in the Treatment of Skin Diseases,” ibid.,
1892, p. 184.
312
INFLAMMA TIONS
course, always be rinsed off with clean water and tapped dry before the
remedial applications are made. Stronger remedies are, however, often
called for; they are essentially the same as indicated in the above types,
but in increased strength. The various lotions, especially of resorcin,
can be employed, with several times as much of this ingredient contained
therein—5 to 20 grains (0.33-1.33) to the ounce (32.); and it can be fol
lowed by a strong salve. The calomel and white precipitate ointments,
already suggested, are often of service, containing 40 to 80 grains (2.65-
5.33) of the mercurial to the ounce (32.); such ointments should be well
rubbed in, but are not applicable to large surfaces for fear of absorption;
for the latter reason their application as a spread ointment, except to a
small area, is not advisable.
Tarry preparations are most frequently of use in these cases, dis
agreeing occasionally; they are most satisfactory in the dry sluggish
types. The mildest of all is the liquor carbonis detergens, already
referred to; as a lotion it can usually be employed strong, even up to
the pure solution, followed by a salve containing it, as before given,
or with the calomel or white precipitate ointment. As a rule, however,
the stronger vegetable tars are usually necessary, such as the oil of
cade or the official tar ointment. The former can be used with 1 or
3 parts of almond or olive oil, or in ointment with simple cerate, 2 to
3 drams (8.-12.) to the ounce (32.). Sometimes a satisfactory method
is to prescribe it with alcohol, 1 to 2 parts, paint over the surface, al
low to dry, and then put on a spread salve application of one of the
mild salves—the salicylated paste is an eligible one. The official tar
ointment should at first be used with 1 to 2 parts lard, and increased in
strength if necessary. In favorable cases the infiltration rapidly dis
appears under the use of these several tar preparation. In limited dry
areas, if not too much thickened, the tar, as the oil of cade, can be in
corporated with collodion, 1 dram (4.) to the ounce (32.), and painted on
two or three times daily for several days, and then under a mild salve
dressing allow the film to come up; the painting can then be renewed.
If the odor of tar is a serious objection, a strong ointment of resorcin
or B-naphthol, or salicylic acid, 30 to 60 or more grains to the ounce,
can be employed at times with great advantage, but, like all other
remedies, they at times disagree. Painting on iodin tincture, at first
weakened with 1 part alcohol, once every few days, is, conjointly with
salves, sometimes of service. The gelatin dressing treatment should
not be forgotten in these cases, as it is often a valuable method; it can
sometimes advantageously be preceded by a shampooing with sapo
viridis and hot water, and sometimes by a preliminary painting with
pure or weakened liquor carbonis detergens.
Occasionally an ointment of sulphur, 20 to 60 grains (1.35-4.) to
the ounce (32.), preferably of the salicylated paste, acts beneficially.
A compound ointment sometimes useful in these thickened sluggish
cases is the following: R. Sulphur, præcip., 3ss-ij (2.-8.); ungt. picis
liquidæ, 3ij-iv (8.-16.); petrolati, q. s. ad 3j (32.). Sulphur must,
however, be used with caution, as it frequently disagrees.
Sulphur, in the more sluggish, obstinate cases, is sometimes used
ECZEMA
313
in the form of sulphur baths, and these, one every two or three days, can,
in some instances, be tried, at least as an adjuvant measure. The
bath is made by adding 1 to 4 ounces (32.-128.) of potassium sulphid to
the ordinary bath-tub about half full (about 30 gallons), the water being
sufficiently warm for the patient to remain in five to fifteen minutes
without being chilled. Tar baths are also occasionally resorted to, the
affected parts being first scantily or freely painted or rubbed with
pix liquida or oil of cade, and the patient then getting in a warm plain
bath. Neither of these methods has found use in my practice in late
years, as favorable effects were so infrequent and irritation or aggrava
tion not unusual. In some cases, however, a course of baths at the sul
phur spring resorts, with the advantages of change of scene, release from
care, supervised diet, and outdoor life, is serviceable.
Other remedies to which recourse must sometimes be had, when
other plans have failed, are ointments of chrysarobin and pyrogallol,
20 to 50 grains (1.33-3.33) to the ounce (32.), but these also must be
cautiously employed. In obstinate cases it is sometimes advisable to
excite inflammatory action, and then follow with soothing applications.
When there is pronounced infiltration of limited extent, which is slow
in undergoing absorption, the cautious application, every few days, of
the negative electrode of the galvanic battery, using 5 to 20 milliam-
pères, will occasionally give the impetus toward recovery. The static
spark is also at times of service in such cases. In some instances the
application of a high frequency current by means of the vacuum elec
trodes, for several minutes or longer, and repeated every few days, has
been beneficial and occasionally curative. The same may be said of the
action of the Röntgen rays; with cautious exposure of three to ten minutes,
with a soft to medium tube, at varying distances of from 3 to 10 inches,
repeated at intervals of several days.
In the treatment of the thickly indurated or sclerosed and verrucous
patches strong applications are, as a rule, necessary to bring about
their removal, or such modification that cure is then possible by the
various plans already named. For reducing these patches there are
several preparations which are of service—chiefly sapo viridis, caustic
potash, and salicylic acid. If at all extensive, a compound of equal
parts of sapo viridis, tar, and alcohol can be used, rubbing it in twice
daily, and allowed to dry on. This can be continued for several days or
longer if no reactive irritation sets in, and then the parts soaked in hot
water, with 1 or 2 drams (4.-8.) of borax to the quart (1000.), and
subsequently thoroughly washed with sapo viridis, rinsed, and dried.
The treatment can be resumed and continued in the same way until
the infiltration is thinned down and the induration removed, or until
irritation is produced, when milder applications can be made. A
cleaner method, and more rapid, but requiring greater caution, is the
use of a solution of caustic potash, ½ to 2 drams (2.-8.) to the ounce
(32.) of water. This is applied carefully, permitted to act a few minutes,
washed off, or its further action prevented by application of vinegar or
dilute acetic acid, and a mild spread salve put on; this is to be repeated,
if necessary, from time to time. A method safer in the hands of those
314
INFLAMMATIONS
less experienced is the application of a 20 to 25 per cent, salicylic acid
rubber plaster, kept constantly applied from one to several days, renew
ing when it loosens. The upper surface of the hardened tissue will be
found softened, and after soaking in hot water, can be rubbed or scraped
off, to be followed by renewal of the treatment until the desired end is
accomplished. A 4 to 10 per cent, paint of salicylic acid in collodion,
painted on twice daily for several days, and then permitted to loosen, and
the part soaked and rubbed or scraped as above, and repeated, will
finally accomplish the same purpose, but usually more slowly. The
imported salicylic acid plaster-mull (Unna) is also valuable for this pur
pose. Papoid and boric acid, in equal parts, with enough glycerin and
water to make a paste, and spread on overnight, will sometimes have a
softening influence on hardened patches. As in other types, treatment by
Röntgen rays can be cautiously tried in particularly obstinate cases.
A preparation sometimes useful in these cases, as well as in some
instances of the chronic sluggish type, is that known as “liquor picis
alkalinus” (Bulkley). It is to be used cautiously, either as a strong
solution with 5 or more parts of water, or as an ointment, 1 to 2 drams
(4.-8.) to the ounce (32.). As a weaker lotion, ½ to 2 drams (2.-8.)
to the pint (500.), it can also be employed in the subacute varieties,
often controlling the itching satisfactorily.1 In extremely rebellious,
thickened sclerous patches the stimulating and superficially cauterizing
action of carbon-dioxid snow (q. v.) can be carefully tried.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |