| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
CLASS II.—INFLAMMATIONS
ERYTHEMA MULTIFORME
Synonyms.—Erythema exsudativum multiforme; Fr., Erythème exsudatif multi-
forme; Erythème polymorphe; Ger., Erythema exsudativum multiforme.
Definition.—Erythema multiforme may be defined as an inflam
matory disease of an acute character, characterized by reddish or pur
plish red, often variegated, macules, papules, and tubercles, occasionally
becoming vesicular or bullous, and occurring as numerous scattered or
grouped lesions of various size and shape.1
Symptoms.—The hands and forearms, especially the dorsal sur
faces, the face, and the legs, particularly on the tibial aspects, are the
most common sites invaded, but it may be more or less extensive. Ex
ceptionally it may be limited to the trunk (Pick, Lewin) and to the face
(Jamieson). It is occasionally of general distribution. The eruption
usually makes its appearance suddenly, and may present itself as ery-
thematous patches of more or less irregular outline and of various forms,
or it may consist almost entirely of small to large pea-sized flattened
papules or tubercles; or the eruption may be of a mixed character. In
most instances, however, there is a predominance of one type of lesion.
In the first few days the lesions are likely to increase somewhat in size,
and new efflorescences appear. In fact, there may be fresh outbreaks
every day or two for five to ten days, when the process begins to decline.
Or the eruption may consist of but one moderate or extensive outbreak,
remain more or less stationary for several days, and then gradually fade.
In color the efflorescences are usually at first of a somewhat bright pink
or red, as a rule becoming later violaceous or purplish, especially in the
papular and tubercular forms of the disease.
1 Some important literature: Lewin (malignant and other forms), Berlin, klin.
Wochenschr., 1876, No. 23, and Charitê-Annalen, 1878, vol. iii, p. 622, Berlin; Schwim-
mer, Die neuropathischen Dermatonosen, p. 101; Düring, “Beitrag zur Lehre von den
polymorphen Erythemen,” Archiv., 1896, vol. xxxv, pp. 211 and 323 (a valuable
exhaustive paper, discursive and analytic, bearing upon infectious, epidemic, and other
characters, with many literature references); Besnier (pathogeny), Annales, 1890, No. 1;
Polotebnoff, “Zur Lehre von den Erythemen,” Unna‘s dermatolog. Studien, 1887, Leip
zig; Molènes-Mahon, “Contribution à l‘étude des maladies infectieuses—De l‘érythème
polymorphe,” These de Paris, 1884, No. 60; Osier, “The Visceral Manifestations of
the Erythema Group” (4 papers), Amer. Jour. Med. Sci., Dec, 1895, and Jan., 1904;
and Brit. Jour. Derm., 1900, p. 227; and Johns Hopkins Hosp. Bull., 1904, vol. xv, p.
259; Schamberg, “An Inquiry into the Etiology and Nature of the Toxic Erythemata,”
Jour. Cutan. Dis., 1904, p. 461; Panichi, “Erythème exsudatif polymorphe,” Giorn.
ital., 1903, pp. 22-179—résumé by the author in Annales, 1904, p. 818 (review, with
report of 16 cases, with histologic examination); Kreibich, Archiv., 1901, vol. lviii,
p. 125 (histologic); “Papers on the Toxic Dermatoses,” by Hartzell, Fordyce, Johns-
ton, and Anthony; and discussion on same, Jour. Cutan. Dis., 1912, pp. 119-167;
“Discussion on Erythema Multiforme,” Brit. Jour. Derm., 1912, p. 427 (paper by
Adamson; discussion by Pringle, Whitfield, Galloway, Macleod, W. Fox, Pérnet,
Morris, and others).
153
154 INFLAMMATIONS
The most common type of the eruption is that which consists pre
dominantly or entirely of papules (erythema papulatum). The papules
are usually small to large pea-sized, flattened, sometimes with a slight
sinking in of the central portion. They may be discrete or crowded
together. They tend to increase somewhat in size, the central part
often becoming depressed and flat, so that some or many of these lesions
have an ill-defined or well-marked ring appearance. In color they
are dark red or violaceous. The most frequent sites of this type are
the dorsal surfaces of the hands and forearms; the legs and feet, and
not infrequently the face also, often share in the eruption. The tuber
cular type (erythema tuberculatum) is similar to the papular, except
that the lesions are somewhat larger and deeper seated, these two types
are commonly seen together. Interspersed nodose lesions, such as dis
tinguish erythema nodosum, are also occasionally associated.
In other instances the larger part of the eruption consists of ery-
thematous patches of various sizes and shapes. Often this type is made
up of distinct rings, constituting the so-called erythema annulare; or,
instead of single rings, the patches may consist of several concentric
rings, the outer rings forming after the inner ones have appeared, and
necessarily, therefore, of different tints of coloring, giving rise to the
term, sometimes employed, of erythema iris. The erythematous erup
tion may, too, present itself as one or several or more extensive spread
ing patches, with a sharply defined border, the older part fading away as
the patches spread at the other side—so-called erythema marginatum.
In some instances in which the eruption consists of rings, these rings
may extend to considerable size and coalesce, the coalescing edges usually
disappearing; there results an eruption of serpentine lines or bands, some
times found described as erythema gyratum.
To a rare and peculiar persistent eruption, partaking somewhat of
the nature of both erythema hyperæmicum and erythema multiforme, and
to a probably still rarer one, partaking largely of the nature of a more or
less general papular erythema multiforme with many of the papules
having the aspects of urticarial lesions, is given the name erythema per-
stans or erythema multiforme perstans. The former type1 consists
usually of erythematous spots or patches, which frequently assume
annular, marginate, and gyrate configuration. The latter type consists
of large pea-sized bright pink or reddish edematous or edematous-looking,
often urticaria-like, solid papules or nodules, often itchy, and with a
tendency to develop into solid elevated segments, gyrate patches, and
rings, some of the latter later breaking up into segments and papules
again; finally, after several months or a year or more, flattening, and
fading slowly away.2
1 G. W. Wende, in his paper (Jour. Cutan. Dis., 1906, p. 241), reporting 2 cases,
gives a review, with references, of other reported cases.
2 One such remarkable instance of this erythema-multiforme-urticaria type has
been under my care recently, the eruption at times quite itchy in character, having
already lasted a year, and slowly and gradually disappearing. The patient had an
exactly similar attack five years previously, which had lasted more than a year. In
looking over the literature, after seeing this case (Phila. Derm. Soc'y Transact., Jour.
Cutan. Dis., 1913), I find that Dr. Pringle (Brit. Jour. Derm., 1912,p. 275, case demon
stration) had recorded a similar instance under the name of urticaria perstans annulata
Plate I.

Erythema multiforme of erythematous and papular type.
ERYTHEMA MULTIFORME 155
In other cases, more especially in the papular and tubercular types,
the inflammatory process may be sufficiently intense as to give rise to
true vesiculation at the central point of the lesions and furnish the clinical
variety, at times designated erythema vesiculosum. In fact, the exu
dation may be sufficiently pronounced to produce distinct blebs—so-
called erythema bullosum. In occasional instances, instead of con
centric erythematous rings, there result concentric vesicular or bullous
rings, forming the herpes iris of some authors; in this type the several
concentric rings being of slightly different duration, the coloring is bril
liant in one, purplish in another, and violaceous in another, hence the
use of the qualifying term iris. The vesicular and bullous rings of a patch
may coalesce and give rise to large and distended blebs simulating the
pemphigus eruption. In cases of the herpetic type the eruption is most
commonly about the hands and wrists, and not infrequently in the palms,
and on the lower part of the legs. Vesicular lesions are also occasionally
found on the lips and in the mouth.
In some cases of erythema multiforme the eruption may be made
up of an admixture of the various types. In extensive cases of the
erythematopapular type the eruption may be more or less general and
seemingly partake of the nature of both this disease and urticaria.
The subjective symptoms are rarely troublesome—frequently en
tirely wanting; in some, slight burning and itching. In the vesicular
and bullous types the patches are often painful. In occasional in
stances, however, especially in those cases having an urticarial element,
the subjective symptoms of burning and itching may be quite intense.
The constitutional disturbance in erythema multiforme is rarely of
any significance. Düring noted temperature-elevation in 31 cases
out of 105; my own observations would place it at even less. Accord
ing to Jarisch, swelling of the lymphatic glands, especially the cervical
glands, is sometimes noted. In some cases, however, especially those
of a general character, there may be a good deal of febrile action, and
often with accompanying swelling and pain about one or more of the
joints. There may also be some anorexia, digestive disturbance, and
malaise. Endocarditis has been noted (Gerhardt) in rare instances.
In exceptional cases of the severe types the febrile action may be quite
pronounced, and continue for several days or longer, or even throughout
the disease. In fact, in some exceptional cases such symptoms may exist
et gyrata. In both these cases the lesions had about the same distribution, hands
and face being practically spared; but in mine the papular or nodular lesions were not
quite so large, being more the size of a large pea to possibly a dime, except, of course,
those which had enlarged by peripheral extension, the center clearing; some of the
rings were 2 to 5 inches in diameter. I rather incline to Dr. Fox's view (article on
“Urticaria,” Clifford Allbutt‘s System of Medicine, vol. ix, p. 214, cited by Pringle) that
“the persistence of a wheal is so contrary to the usual temporary character that we
rightly assume a critical attitude in accepting an “urticaria perstans”; and for that
reason and also for the reason that distinct spreading rings are rarely, if ever, seen in
true urticaria, I believe it more appropriate to class this rare eruption as an “erythema
multiforme perstans,” although confessedly such a long persistence of the lesions of
erythema multiforme is almost equally as anomalous. Many of the papular or nodular
lesions in these cases are in their objective characters, however, very much like the
wheals of urticaria. Graham Little also describes (ibid., 1912, p. 119—case for diag
nosis) a case with some features in common with those just referred to.
156
INFLAMMATIONS
a few days before the eruption appears (Rigler, Lipp, Lewin, Düring, and
others). The observation has been occasionally made also that in some
instances the cutaneous lesions are preceded by an inflamed or congestive
or eruptive condition of the fauces (Solstier, Boeck, Jamieson, Fuchs), or
less frequently a mild conjunctivitis (Fuchs, Düring). Exceptionally,
too, the lips and mouth show vesicles or blebs before the skin is involved
(Pringle, Crocker). Grave cases of erythema multiforme have been
reported (Lewin, Gerhardt, Osier, and others), with visceral involve
ment or complications of considerable severity, and in some of which
purpuric symptoms presented. In these cases, among other symptoms
were noted throat complications (Osier), diarrhea and colic (Galliard),
endocarditis (Gerhardt), and laryngeal symptoms (Cotte). It is difficult
to place such cases, but they probably belong either to a serious systemic
infection of which this eruption is but a part, or they (some of them)
belong to the domain of purpura. Other cases in which the eruption
became rapidly bullous, and continued more or less as such, with some
times a fatal termination—being, I believe, more of the nature of a septic
pemphigus.1 Certain it is that in average cases, and especially those of
the papular type, in which the eruption is limited to the hands and fore
arms, face, and possibly the legs, there are no perceptible systemic symp
toms. In fact, the disease ordinarily is benign, and runs an acute course.
Etiology.—The disease is not uncommon, constituting between
0.5 and 1 per cent, of all cases. The causes which lead to erythema
multiforme are still obscure. My own experience would give weight
to the belief that the development of intestinal toxins, and probably
toxins from other sources, is an all-important factor in many cases.2
Stale articles of food, especially meats, oysters, fish, crabs, and lobsters,
are, I believe, often causative. On the other hand, the more severe and
rare grave types are thought to be of an infectious nature (Lewin,
Molénes-Mahon, Vidal, Leloir, and others); in support of which are
quoted epidemics (Rigler, Gaal, Herxheimer, Düring) and the various
bacteriologic findings in the blood (Cordua, Luzzato, Manssurrow, Le-
grain, Simon, Haushalter, Leloir, Finger, and others). As already
intimated, in these grave cases the erythema multiforme is probably
only a part or one of a group of symptoms of a general toxemia or infec
tion. As yet, however, there has been no uniformity in the micro-
organisms found.
There are certain facts generally recognized in association with
this disease. It is more frequently observed in the spring and autumn
months, during which seasons atmospheric conditions are somewhat
variable, and the weather often damp and rainy. It is apt to recur
for one or two years. Moreover, there are not infrequently associated
1 Corlett, “Erythema Exudativum Multiforme,” Jour. Cutan. Dis., 1908, p. 7,
with a report of a case of erythema circinatum bullosum et hæmorrhagicum, following
a gunshot wound, apparently due to streptococcus infection, and terminating fatally,
reviews these grave cases with full bibliography.
2 Thus is doubtless explained the cases seen occasionally in the course of such
diseases as typhoid fever, diphtheria, etc.; Parker and Hazen, “Erythema Multiforme
During the Course of Typhoid Fever,” Johns Hopkins Hosp. Bull., March, 1911,
briefly review these cases, with references.
Plate II.

Erythema multiforme of bullous variety, in a young woman, on the dorsal surfaces
of the hands and forearms symmetrically ; in places a central bleb, surrounded by outer
ring-shaped bulla—a tendency to “herpes iris.” Duration, eight days.
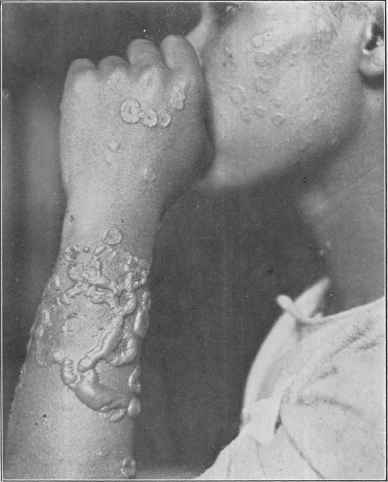
Erythema multiforme of erythematovesicular, circinate, and bullous varieties, in a
young mulatto woman, of one week's duration. The bullæ on arm have coalesced,
forming serpiginous tracts. Eruption occupies the face and the forearms and hands
symmetrically.
ERYTHEMA MULTIFORME
157
rheumatic symptoms. It is common to both sexes, but is somewhat
more frequent in females; all ages are liable, but it is most frequent
during adolescent and early adult life. It is also noted that newly
arrived immigrants and young servants coming to city-living from the
country (Tilbury Fox) are especially prone to it. Another possible
etiologic factor not to be lost sight of is drug-action; it has followed
the administration of such drugs as potassium iodid, copaiba, some of the
coal-tar group, and others. Antitoxin and other serums are sometimes
causative.
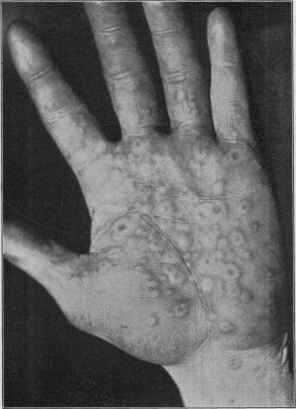
Fig. 27.—Erythema multiforme bullosum—herpes iris.
Tn recent years the suggestion has been advanced that this and other
toxic dermatoses may be due to the absorption, commonly from the
intestinal tract, of imperfectly digested or improperly broken up proteid—
in short, due to anaphylaxis or hypersensitiveness to a foreign albuminoid
substance (see Urticaria).
Other factors also seem to have an influence. Urethral irritation
(Kaposi, Lewin) and in women uterine disturbances have been looked
upon as of etiologic importance (Hebra, Pick, and others). Besnier
believes there must be in all cases an underlying neurotic basis. Urine
examinations give no insight into the cause.
158
INFLAMMATIONS
Pathology.—Erythema multiforme is a mildly inflammatory dis
order, somewhat similar to urticaria, due doubtless primarily to some
impression upon the nervous system, and secondarily upon the periph
eral circulatory system; in short, an angioneurosis (Landois, Lewin,
Auspitz, Schwimmer). It would seem probable, from the presence of
organisms in the blood demonstrated in several instances, already
referred to, and to the fact that some cases seem due to spoilt food, that
the vasomotor disturbance which gives rise to the lesions must be of toxic
origin; in other words, that the disease is a toxic angioneurosis (Claisse
and Legendre); the toxin possibly of diverse character. It is probable
that it may act either centrally or peripherally. The association with
rheumatism noted has led many to believe that it is due to the same
underlying cause (Bazin, Boeck). The fact that extravasations of
blood are occasionally observed in the lesions has led to an expression of
belief that it is a form of purpura (Bohn, Legrand, Purdon, and others);
and the grave cases reported (Osier and others) are strongly suggestive
in this direction, as already referred
to. The characters of the cutaneous
lesions are determined by the amount
of exudation, which is variable. The
first step is doubtless a simple hyper-
emia due to vascular dilatation, fol
lowed by a paresis of the cutaneous
vessels, arterioles, and capillaries, with
cell proliferation and edema.
The anatomy of the process has
been clearly presented by the studies
of Leloir, Lewin, Villemin, Unna,
Jadassohn, Crocker, Gilchrist, Pardee,
and others. As is to be expected, the
epidermic changes are more marked
in the vesicular and bullous lesions.
The papillary layer is the seat of
the principal inflammatory changes,
consisting of dilatation of the vessels,
around the walls of which are found
cell proliferation, cell emigration, and
edema of the cutis, and sometimes extravasation of red corpuscles and
colored blood-serum. The epidermis shares in the edematous infiltra
tion; this edema reaches generally from the subepithelial vascular net to
the epidermis, and doubles or trebles the thickness of the papillary layer
(Unna). The migratory cells are to be found in more or less abundance
in the upper rete layers (Cornil and Renaut). The covering of the
vesicles and bullæ, as in similar lesions in other diseases, consists of the
corneous layer, sometimes of the entire epidermis (Pardee). Kreibich
and Panichi, from their histologic studies, believe the disease should be
regarded as an inflammatory dermatitis rather than as an angioneurosis.
Diagnosis.—The diagnosis of erythema multiforme rarely gives
rise to serious difficulty if the multiformity of the eruption, the size

Fig. 28.—Erythema multiforme bul-
losum—herpes iris.
PLATE III.
Erythema multiforme—erythema and herpes iris—of unusually extensive development,
some of the patches consisting of six rings and of varied coloring. (Case reported in
Medical Nezvs, October 14, 1882.)
ERYTHEMA MULTIFORME 159
of the papules, frequent tendency to ring shape, the frequent limitation,
especially of the papular type, to certain parts, the course of the disease,
and the entire or relative absence of subjective symptoms are con
sidered. It resembles urticaria to some extent, but the lesions of this
latter disease are evanescent, disappearing and reappearing in the most
capricious manner, and are usually whitish in the central portion. The
papules of erythema multiforme persist for several days at least, and
usually a week or more. Moreover, urticaria, is intensely itchy and
the eruption is most pronounced, as a rule, upon covered portions of the
body, especially about the buttocks and lower lumbar region and shoul
ders. The papules of erythema multiforme are usually somewhat dark
colored, with a tendency to take on a purplish or violaceous hue, and
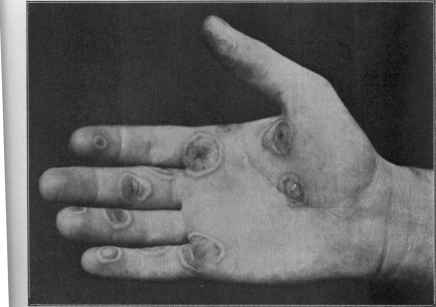
Fig. 29.—Erythema multiforme bullosum—herpes iris.
often with a slight depression of the central portion. Those types of
erythema multiforme characterized by distinct rings can scarcely be
confounded with any other disease; ordinary care would serve to dis
tinguish it from ringworm, to which it bears rough resemblance. This
latter disease has usually a scaly or papular border, and a slightly scaly
center; moreover, rarely more than a few patches are present.
In those cases of vesicular and bullous types in which, from con
fluence of the vesicles and small bullæ, distinct blebs arise, may be
confused with pemphigus, but the distribution of the eruption and the
method of formation of the bullæ, and usually the presence of some
characteristic erythema multiforme patches, will serve to differentiate.
It can scarcely be mistaken for erythema nodosum; in this latter disease
the location of the eruption and the size of the lesions and color will
furnish sufficient points of difference.
160 INFLAMMATIONS
Prognosis.—This is, as judged by the observations of all American
dermatologists, practically always favorable, in average cases the erup
tion disappearing in from ten days to several weeks, and without per
manent trace. The graver cases are apparently more frequent in
Europe. In some instances, however, new crops may appear from
time to time for a month or more, and the course of the disease be pro
longed. One or more recurrences in succeeding years are not uncommon.
In exceptional cases, especially of the vesicular and vesicobullous type,
in which the mouth and lips are sometimes involved, frequent and
closely connected recurrences may give the disease almost a chronic
aspect; and it may, in fact, last for months and years (Bazin, Kaposi,
Hutchinson, Polotebnoff, Colcott Fox, Payne, and others). These cases,
in which there may be troublesome itching, more properly belong, how
ever, to dermatitis herpetiformis.
In those rare and grave cases referred to in which the eruption is
doubtless a part of a general systemic disease, or distinctly infectious,
the prognosis would depend upon the character and gravity of the
constitutional involvement. I have never met with this grave type,
except in one or two instances when the eruption was simply a comani-
festation of septicemia; others (Uffelmann, Vidal, Leloir, and others)
have, however, recorded deaths, usually from visceral involvement or
complication.
Treatment.—It is difficult to state how far treatment influences
the course of the disease, but that it has no effect whatsoever, as many
contend, is not in accord with my own observations. As it is probable
that the development of intestinal toxins plays an important rôle in many
of these cases, the treatment most commonly to be prescribed, and which
in my experience is the most satisfactory, should consist of such remedies
as sodium salicylate, salol, thymol, and sodium benzoate, in fairly full
dosage. Conjointly with one or more of these an occasional laxative
dose of calcined magnesia should be given. In fact, saline laxatives alone
are often sufficient. Of these, magnesium sulphate and sodium phos
phate are the most satisfactory; or the well-known laxative mineral
waters may be substituted. In the more stubborn cases large repeated
doses of quinin sometimes prove of benefit. Probably the remedies
most frequently to be prescribed in this disease are salol or sodium
salicylate, with small doses of charcoal and an occasional laxative dose of
calcined magnesia, or they may be prescribed in combination as follows:
R. Pulv. salol., gr. xx (1.35);
Pulv. magnesiæ calcinat.,
Pulv. carb. ligni, ââ gr. xl (2.65).
To be divided into 20 parts and put in capsules. Of these, one is to be
taken every three or four hours—about four daily.
In those cases in which rheumatic swellings and pains are present,
sodium salicylate in full doses, with an occasional saline purge, will
give the most prompt relief. In those constantly recurring cases in
which the lips and mouth are coinvolved particular attention should
be given to the condition of the digestion, and intestinal antiseptics,
along with arsenic, should be administered, with other remedies which
ERYTHEMA NODOSUM
161
might be called for by some special condition of the patient; continued
doses of quinin, arsenic, iron, and strychnin, and, in some cases, cod-
liver oil, will prove of service. Among other remedies advised may be
mentioned salicin (Jamieson), potassium iodid, 30 grains daily (Villemin,
Elliot), more especially in the vesicular and bullous types (Elliot);
for the relapsing and frequently recurring forms, quinin (Duhring, Pelon,
Payne) and ergotin (Schwimmer).
As a rule, external treatment is, in the simple erythematous and
papular manifestations, rarely required. In the more or less generalized
cases, however, especially those in which the disease presents an urticarial
aspect, with burning and itching, antipruritic applications, such as are
employed in urticaria, may be advisable.
The larger vesicular and bullous lesions should be punctured, and
the contents gently pressed out. In these latter cases the “calamin-
zinc-oxid” lotion, named under the head of Eczema, may also be em
ployed with advantage, or one of the mild soothing ointments can be
applied, spread on lint. In those patients in whom erythema multi-
forme tends to recur yearly a course of intestinal antiseptics and occa
sional purgation, previous to the usual time of the outbreak, together with
the avoidance of dietary indiscretions, will, I believe, sometimes ward off
the attack.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |