| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
IMPETIGO CONTAGIOSA
Synonyms and Varieties.—Porrigo contagiosa; Impetigo parasitica; Impetigo
vulgaris (Unna); Impetigo simplex; Impetigo sparsa; Impetigo streptogenes; Impetigo
staphylogenes; Impetigo circinata; Impetigo figurata.
Definition.—Impetigo contagiosa is an acute, contagious, inflam
matory disease, characterized by the formation of discrete, superficial,
flattened, rounded, or oval vesicles or blebs, often becoming seropurulent,
and drying to thin yellowish crusts.
Exceptionally the beginning lesions are small pustules, and which
may dry to thicker crusts. And occasional types of a circinate or even
serpiginous configuration are noted.
Symptoms.—In a typical case of impetigo contagiosa of the
common form of the disease several vesicopapules, vesicles, or ves-
icopustules make their appear
ance simultaneously or in rapid
succession upon the face, face
and scalp, or face and fingers,
or upon all these various parts.
At first small, they tend to in
crease in size, becoming de
cidedly flattened, with, in some
cases, in some of the lesions, a
slight relative depression of the
central part, as compared to
the extending peripheral por
tion ; there may even be distinct
umbilication. They are super
ficial, and, as a rule, are without
conspicuous areola and without
distinctly inflammatory base.
They attain the diameter of a
pea or a dime, and when close
together, as often noted when
about the mouth and chin,
coalesce and form one or more
large, irregular patches. The
contents at first are often purely serous, later becoming milky or
seropurulent or even purulent. If a vesicopustule or bleb is broken,
a reddish, moist, abraded-looking surface is exposed, secreting a thin
watery or puriform liquid, and looking not unlike a superficial burn or
abrasion. Several days after the appearance of the lesions they begin
to dry to thin, granular, yellow or yellowish, wafer-like crusts, which
are but slightly adherent, and later on, when the edges have com
menced to loosen, have the appearance of being imperfectly pasted

Fig. 99.—Impetigo contagiosa in a girl of
ten years, of one week‘s duration, crusting
stage already reached; on chin and nose
lesions have coalesced.
398 INFLAMMATIONS
on. A not unusual site for a vesicopustule is around a finger-nail,
where it is somewhat suggestive of a superficial paronychia. Excoria
tions, scratch-marks, or abrasions, if present, soon become, through
auto-inoculation, the seat of characteristic lesions. Fresh lesions may
appear singly or in crops from day to day, but finally, in the course of
several days or a week, new ones cease to form and the malady gradually
ends. The crusts soon drop off, leaving behind reddish spots which
rapidly fade away. Itching may or may not be present. The whole
course of the disease, as a rule, occupies ten days to a few weeks.
Occasionally, in addition to the eruption upon the skin, the conjunc-
tival, nasal, or oral mucous membranes may show lesions; and excep
tionally the greater part of the eruption may be about and in the
nasal orifices and about the lips, and even within the mouth.1 As a
rule, there is no constitutional disturbance, but when the eruption is
extensive, as it is more apt to be in the epidemic form of the disease,
it is preceded by light febrile action and malaise.
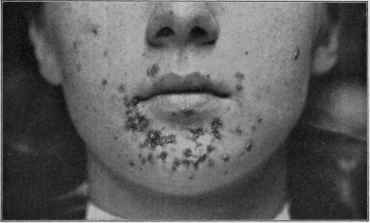
Fig. 100.—Impetigo contagiosa, with small lesions, in a girl of fourteen years, and of
six days’ duration.
All observers have recognized the existence of anomalous types.2
In some of these the eruption consists of but two, three, or several
ill-defined lesions about the nose and mouth, with possibly one or two
upon the fingers. In others, again, the eruption is more or less scattered
1 D. W. Montgomery, “The Determination of Impetigo Contagiosa to the Mucous
Membranes,” Jour. Cutan. Dis., 1910, p. 445; Cushing, “Stomatitis in Impetigo
Contagiosa,” Arch. Pediat., June, 1904 (with literature references); Cornby, La France
Medicale, Dec. 24, 1887 (cited by Cushing) records instances of vulvovaginal involve
ment.
2 Foster, “Herpes Contagiosus Varioliformis,” Arch. Derm., 1875, p. 97; Corlett,
“Impetigo: Its Clinical Forms and Present Status, Including Ecthyma and the so-
called Pemphigus Contagiosus,” Cleveland Jour. Med., 1898, vol. iii, p. 513; Allen
(general—bullous), Trans. Amer. Derm. Assoc. for 1896; Elliot (general—bullous),
Jour. Cutan. Dis., 1894, p. 194; Anthony (various forms), ibid., 1898, p. 218; Stel-
wagon (various forms), Phila. Med. Times, Sept. 22, 1883; Engman, “Impetigo Con-
tagiosa and Its Bacteriology,” Jour. Cutan. Dis., 1901, p. 180 (with review and bibli
ography); Grindon (bullous), ibid., p. 188.
IMPETIGO CONTAGIOSA
399
over face, hands, limbs, and to a less extent upon the trunk. In some
instances, of more or less general distribution, the lesions, instead of
being flat, consist of pea- to nut-sized blebs, flaccid or tense; and when
occurring in an epidemic manner among infants and young children the
malady simulates, according to the predominant size of the lesions,
varicella or pemphigus (impetigo contagiosa bullosa). Most, and proba
bly all, of the reported cases of contagious pemphigus and acute pem
phigus in infants and children are examples of this variety (impetigo
streptogenes?); and exceptionally such cases assume a serious aspect.
In occasional cases they may present segmental or ring-like or ser-
piginous configuration (impetigo circinata, impetigo figurata).1 In rare
instances, instead of vesicles or blebs, many of the lesions are pustular,
and especially those upon the legs, ecthymatous, with a markedly in
flammatory base and areola. Exceptionally, as in the variety described
by Duhring2 as impetigo simplex (impetigo staphylogenes), the vesicular
stage of the disease seems to be wanting, the lesions appearing as pure
rounded globular pustules, with little or no tendency to flattening; and
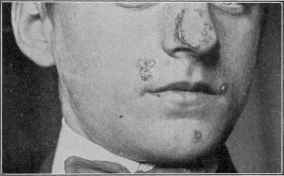
Fig. ioi.—Impetigo contagiosa of slight development and showing a circinate patch; of
six days’ duration, in a youth of eighteen. Crusting stage already reached.
which, in some cases, may, instead of developing into ordinary matured
impetigo lesions, lead to deeper invasion by the organisms and to boil
formation. As Bockhart has shown in this type, the lesion is usually
follicular. It is seen not infrequently about hairy regions, as the nape
of the neck, about the ankles, and other general surface regions in hairy
individuals; and in those cases in which the lesions are close together and
almost coalescent could be clinically well described as a pyogenic derma
titis (dermatitis pyogenica, pyodermia, pyodermatitis, pyodermitis).
It is probable that the rare condition, vacciniform ecthyma of infants,3
is of the nature of impetigo contagiosa; it usually involves the genitocrural
1 See remarkable case by Schamberg, Jour. Cutan. Dis., 1896, p. 169 (with illustra
tions).
2 Duhring (a report of 2 typical examples), Amer. Jour. Med. Sci., Oct., 1888;
also Leslie Roberts (1 case), Brit. Jour. Derm., 1895, p. 142.
3 Colcott Fox, “Vacciniform Ecthyma of Infants,” Brit. Jour. Derm., 1907, p. 191
(with several illustrations), reports some cases, and reviews the subject, with references;
Halle, Dermatolog. Zeitschr., 1908, p. 215 (with colored plate).
400 INFLAMMATIONS
and anal regions. It begins, as a rule, as one, several, or more small
papulovesicular elevations on an erythematous base; the vesicular nature
is soon manifest, the vesicles becoming larger, flattened, and somewhat
superficial, and with central depression, giving the lesions a distinctly
vacciniform aspect. Coalescence may occur here and there, resulting
in the formation of an irregular surface, or crusted, granulating, eroded,
or diphtheroid areas. Sometimes the developed lesions become eroded,
and with the slight seropurulent secretion on moist surfaces resemble the
eruption of syphilis seen in this region in infants. The intervening skin
may be erythematous in its entirety or in spots, the color being of some
what dark shade.
In exceptional instances the common sites for impetigo contagiosa
may share only slightly in the eruption, or may be entirely exempt,
the lesions appearing in unusual regions.1

Fig. 102.—Impetigo contagiosa of the ring-like type not infrequently seen in the bearded
region of the male adult (courtesy of Dr. H. K. Gaskill).
When seen occurring in adults the eruption consists usually of a
few abortive lesions on the face or hands; in some cases, however, it
presents numerous discrete and closely crowded pea- to dime-sized
or slightly larger lesions about the bearded region and the neck, and which
quite frequently show a distinct tendency to ring-like development, the
serous and seropurulent formation is often quite scanty, and in such cases
the lesions may show considerable resemblance to ringworm patches.
This more extensive variety is met with in the male adult and is com
monly contracted in barbershops.
1 In 103 cases observed at the Philadelphia Dispensary for Skin Diseases the site
was as follows: Face, 49; face and hands, 12; face and limbs, 6; face and scalp, 5; face,
scalp, and hands, 5; face, hands, and other parts, 4; face and trunk, 3; face and but
tocks, 3; face and feet, 1; legs, 3; trunk and legs, 2; trunk and limbs, 1; hands and
neck, 1; hands and buttocks, 1; scalp, 1; buttocks, 1; limbs, 1; distribution more or
less general, 4.
IMPETIGO CONTAGIOSA
40I
According to Unna,1 the chief differences between the common type
observed (his impetigo vulgaris—impetigo contagiosa of T. Fox) and
impetigo circinata, impetigo staphylogenes, and impetigo streptogenes
are: in impetigo circinata there are no thick crusts, but scales containing
more horny cells than serum, and the lesions spread at the borders, form
ing discoid and gyrate figures, clearing in the central portions. In
impetigo staphylogenes (of Bockhart) the lesions are small pustules with
an areola, and are discrete for some time before coalescing, and lead to
the formation of comparatively small and thin crusts; the lesions do not
remain long as impetigines, but the staphylococcus, by invading the hair-
follicles, leads to folliculitis,
furuncles, whitlows, etc Im
petigo strep togenes lesions
commence with serous exuda
tion, giving rise to flaccid bullæ,
generally large in size, and with
grayish-yellow, turbid contents.
If the experience of other
observers is at all similar to
mine, there are instances met
with in which the characters
of these several types are
found in the same case; Sa-
bouraud‘s investigations dem
onstrate the possible admix
ture of two types, primarily
to invasion of streptococci,
secondarily to staphylococci.
Etiology,—The disease
is contagious in all its forms,
inoculable and auto-inoculable.
From its occasionally occur
ring in epidemics it would al
most seem as though the
malady might in some in
stances be infectious. It is
observed commonly in the
lower ranks of life, although
it is not infrequently seen among the wealthier classes. It is largely
a disease of infancy and early childhood, being most common between
the ages of two and ten; in recent years however a steady increase has
been noticeable among older subjects in our preparatory schools and
colleges. In men, occurring about the bearded region, it is usually
contracted in barbershops. Epidemics have also been noted to occur
among youths and adults through interchange of apparel or the use
of common or insufficiently cleansed towels, as with football players
(football impetigo), in schools, and among bathers (bath-house impetigo)
at the shore.
1 Quoting from the abstract of his paper (loc. cit.) in Brit. Jour. Derm., 1899, P- 332.
26
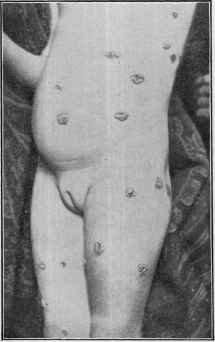
Fig. 103.—Impetigo contagiosa in a child
of three, and of five days’ duration. Lesions
scattered, and more of the nature of the type
of “impetigo simplex” described by Duhring.
402
INFLAMMATIONS
A relationship to vaccination1 has been noted in some instances, but
the same relationship may be said to exist, I believe, to other suppurative
processes or lesions. It is also seen in association with pediculosis and
scabies; the minute punctures made by the parasites and the excoriations
produced by scratching furnishing opportunity for the necessary inocula
tion.2
Pathology.—It is known that the disease is due to pus-cocci,
staphylococcus aureus, streptococcus and possibly the staphylococcus
albus. As intimated in the preliminary remarks, other cocci are doubt-
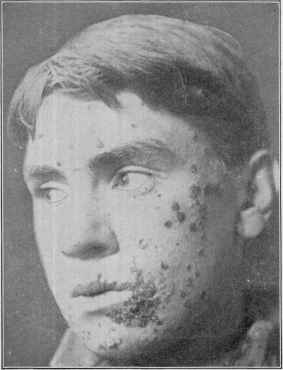
Fig. 104.—Impetigo contagiosa of the male adult, of bearded region and of about a
week's duration, showing discrete and confluent lesions; usually contracted in barber
shops and presenting lesions more especially on bearded parts of the face and neck, and
which are frequently ring-like in character (courtesy of Dr. J. F. Schamberg).
less also etiologic; and it has been alleged by Unna that the various
forms have each a specific coccus, but this needs further confirmation.
The general belief3 is that it is a staphylococcic affection with a disposi-
1 Stelwagon, “Impetigo Contagiosa: Its Individuality and Nature,” Medical News,
Aug. 29, 1883 (out of 88 cases, in 6 only did it follow vaccination; others have, how
ever, observed this association in larger proportion. This paper contains most litera
ture references to date).
2 See paper by Klotz on “The Infected Scratch and Its Relations to Impetigo and
Ecthyma,” Jour. Cutan. Dis., 1896, p. 46.
3 Dr. C. J. White, “The Rôle of the Staphylococcus in Skin Diseases,” Trans.
Mass. Med. Soc'y for 1899, gives a good brief review of this question.
IMPETIGO CONTAGIOSA
403
tion to view the other findings as accidental; although French observers
for the most part, incline to consider the earliest invasion streptococcic,
which is soon concealed or overwhelmed by staphylococci.1 Excep
tionally the ringworm or other fungus will provoke somewhat similar
lesions (Kaposi, Piffard, Colcott Fox, Geber). Crocker2 was the first
to demonstrate clearly that the disease was due to a coccus, and the in
vestigations by Unna and Sabouraud, if carefully examined, appear, in
fact, to corroborate the correctness of these earlier findings as the cause
of some cases of the disease. In some instances—those in which the
eruption is epidemic and more or less general in its distribution, and,
more especially, the bullous type, with slight constitutional disturbance
—the disease certainly bears resemblance to such eruptive fevers as
varicella; it is difficult, it is true, to reconcile such examples with the
numerous simple cases of undoubted pus-inoculation lesions occurring
about the nose, mouth, and hands.
The lesion is formed (Robinson, Unna, Gilchrist, and others) between
the rete and horny layer, this latter being the roof-wall; there is a sur
rounding mild inflammation. The underlying upper part of the corium
displays acute inflammatory action, with the usual features. The
lesion contains polynuclear leukocytes in large number, some round
mononuclear cells, a few detached epithelial cells, small quantity of
fibrin, and a large quantity of coagulated albumin (serum), and, especially
in the central portion of the lesion, a large number of the staphylococcus
pyogenes aureus, often streptococci, as well as sometimes other cocci.
Diagnosis.—Impetigo contagiosa is to be differentiated from pus
tular eczema, ecthyma, varicella, and pemphigus. The patches formed
by coalescence bear, it is true, a rough resemblance to pustular eczema;
but this latter is accompanied with other symptoms of eczema, such
as more or less infiltration and thickening of the involved skin, with
intense itching. Moreover, in impetigo contagiosa discrete lesions are
always to be found, and these differ from the individual pustules of
eczema in greater size, in the absence of a tendency to rupture, and their
course.
Impetigo contagiosa differs from ecthyma by the absence of the
inflammatory base and areola. The distribution is also unlike the erup
tion in the latter malady, being ordinarily upon the face and hands or
face and several other parts, while that of ecthyma is commonly seated
upon the legs. Moreover, impetigo contagiosa is essentially a disease
of childhood, whereas ecthyma is usually observed in adults. In the
former, too, the process is superficial and the crusts are thin; in the latter
deep-seated, and the crusts are thick.
The lesions of varicella are uniform and smaller, rarely larger than
split peas, and more or less disseminated, with no tendency to patch-
formation and with insignificant crusting. In those rare cases of im-
1 Dubreuilh and Braudeis, “Note on the Bacteriology of Pyodermatitis,” Annales,
June, 1910, p. 323; British Jour. Derm., 1911, p. 91, cannot confirm Sabouraud‘s
dictum—“all types beginning with a vesicle or bulla due to streptococci, those beginning
with a pustule staphylococcus;" but believe it is sometimes one, sometimes the
other, and in some cases mixed.
2 Crocker, Lancet, 1881, vol. i, p. 82.
404
INFLAMMATIONS
petigo contagiosa resembling pemphigus the disease must be studied
in its entirety, and sometimes for several days before it is possible to
be positive as to diagnosis. Pemphigus is exceedingly rare. In true
pemphigus the lesions spring from the sound skin usually as blebs
of some size from the start, whereas in impetigo contagiosa they are
small in the beginning and grow in size by peripheral extension.
The eruption of pemphigus has no parts of predilection, and, more
over, is generally accompanied by symptoms of constitutional dis
turbance. In impetigo contagiosa some of the characteristic lesions
are usually present, or frequently another member of the family will
present the typical disease.
Prognosis.—The effect of treatment is, as a rule, prompt; indeed,
impetigo contagiosa in most instances tends to spontaneous disap
pearance in ten days to a few weeks; but in exceptional cases, more
especially in those in which itching is present to a sufficient degree to
lead to scratching, the excoriations thus made become inoculated, and
in this manner the disease, unless actively treated, may persist for one
or two months. A pediculosis capitis is also at times a causative factor
in prolonged cases.
Treatment.—Treatment consists in the destruction of the auto-
inoculable properties of the crusts and contents of the lesions. The
crusts should be removed by warm water and soap washing, fresh or
distended lesions being first opened. An ointment of 10 to 20 (0.65-1.35)
grains of ammoniated mercury to the ounce (32.) of cold cream or petro
latum should then be gently but thoroughly rubbed into the secreting
base of the lesions two or three times daily. When the crusts are quite
adherent and fail to come off with ordinary washing, the salve just
named should be applied over the patch, and the washing and such
anointing repeated two or three times daily until the crusts come away,
after which the ointment should be rubbed into the secreting base.
In many of these latter cases, indeed, partial or complete healing will
be found to have taken place beneath the crusts. In some instances
a drying salve such as Lassar's paste with the addition of the white pre
cipitate or 20 to 30 grains (1.33-2.) of sulphur to the ounce (32.) is
more satisfactory. Any mildly antiseptic ointment will, however, be
found curative.
In markedly itchy cases, in which the disease tends to continue
from inoculation of the scratch-marks thus provoked, a lotion of the
saturated solution of boric acid, with 5 grains (0.33) of either carbolic
acid or resorcin, or both, to the ounce (32.), should, as a preventive
measure, be applied two or three times daily to the affected parts gener
ally. Ordinarily in all extensive cases this lotion can be advised along
with the salve as a routine measure. For lesions occurring on the con
junctiva a plain boric acid lotion, 10 grains (0.65) to the ounce (32.),
may be dropped in the eye once or twice daily.
In those cases of more or less general distribution, in which mild
febrile action is present, in this respect resembling slightly the erup
tive fevers, a laxative should be given and the patient kept at com
parative rest for a day or two; in other respect, the treatment is the same.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |