| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
PITYRIASIS ROSEA1
Synonyms.—Pityriasis maculata et circinata (Bazin); Herpes tonsurans macu-
losus (Hebra); Fr., Pityriasis rosé.
Definition.—A mildly inflammatory affection, characterized by
discrete and frequently confluent, plain or circinate, salmon tinted,
pinkish or pale red, variously sized, slightly raised, scaly efflorescences,
seen most abundantly upon the trunk.
1 Early literature: Gibert, Traité pratique des maladies de la peau, Paris, 1860, p.
402; Duhring, “Pityriasis Maculata et Circinata,” Amer. Jour. Med. Sci.. Oct., 1880;
Behrend, “Ueber Pityriasis rosea (Gibert), maculata et circinata (Bazin),“ Berlin,
klin. Wochenschr., 1881, p. 552; Colcott Fox, “On the Disease of the Skin named
Pityriasis Maculata et Circinata,” Lancet, Sept. 20, 1884, p. 485.
PITYRIASIS ROSEA
195
Symptoms.—The trunk, and especially laterally, usually first
shows the eruption. It may appear rapidly and attain full development
in the course of several days; or its appearance may be slow and gradual,
coming out irregularly or in several distinct crops, one to two weeks elaps
ing before its acme is reached. In some cases, as Brocq1 has pointed out,
the affection is heralded by a primary, somewhat large, efflorescence,
which is seen most frequently anteriorly near the middle of the waist,
and this is the forerunner of the more or less generalized eruption, which
appears from four to ten or twelve days later. The lesions are, as a rule,
but slightly elevated, well or irregularly rounded or oval macules, and
with trifling or moderate scaliness. They vary in size from a small pea
to a silver quarter, are usually quite numerous, pinkish or pale red in color,
and often, especially toward the period of defervescence, present a distinct
salmon tinge. The eruption may be scanty, consisting of thirty to sixty
or seventy patches, or, as more commonly occurs, is quite abundant.
The scaliness is somewhat variable, usually slight, but in occasional in
stances in some of the lesions may be quite pronounced. As a rule,
however, the lesions do not remain, as just described, but some or many
of them spread peripherally and become less marked centrally, present
ing a circinlate patch; the central part is noted to be but slightly involved,
while the periphery, by its more pronounced scaliness, is quite distinct.
In many cases the circinate character presents only after the disease has
lasted for several days or longer; in others it is a part of the eruption from
the start. The scaliness is rarely abundant in these latter cases, but usu
ally bran-like or flaky, and of a gray or dirty-gray color, and in ,a major
ity of cases most marked peripherally. As the circinate patches extend,
the central portions are gradually clearing up, and several or more some
times coalesce and form large irregular areas. The skin is rarely thick
ened, shows practically no infiltration, the process being usually super
ficial. The color of the patches varies somewhat in different cases, in
this respect there seeming to be two or three varieties: in one grayish
with a faint reddish or pink tinge, in another somewhat similar to that of
parakeratosis psoriasiformis of Brocq, and in the other a rather striking
salmon, sometimes coppery, color, suggestive of a syphilid. In short,
pityriasis rosea not only in this particular, but also in extent, character,
duration, varies considerably in different cases, in some instances even
presenting a close resemblance to an extensive dermatitis seborrhoica.2
The eruption may be limited to the trunk, or trunk, neck, upper
arms, and thighs; exceptionally it is of wider distribution. The face
is not often involved. After one or two weeks, in average cases, the
eruption begins to decline, and in the course of several weeks, or at the
most a few months, it has entirely disappeared. Exceptionally, it is
somewhat slower in its course. Slight itching may be present, espe
cially when the patient is warm or perspires, but in most instances there
is an entire absence of subjective symptoms. As a rule, there is no
1 Brocq, “Note sur la plaque primitive du pityriasis rosé de Gibert,” Annales, 1887,
p. 615.
2 In a paper well illustrated G. H. Fox, Jour. Amer. Med. Assoc, Aug. 17, 1912,
called attention to the fact that the disease is not always of a single, clean-cut type.
196
INFLAMMATIONS
constitutional involvement, although in extremely extensive cases there
may be at the outset slight general disturbance of mild character.
Etiology.—The disease is rather infrequent. It is met with in
both sexes, and almost at any age, but is more common in grown children
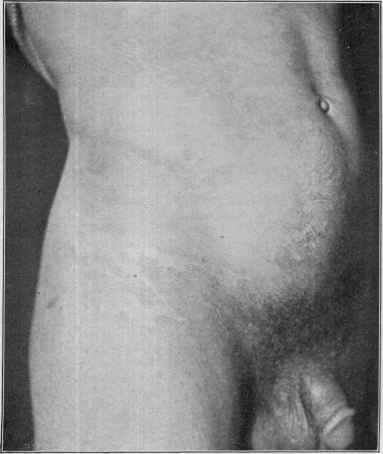
Fig 37-—Pityriasis rosea in an adult aged thirty, of two weeks’ duration, and in
volving trunk, upper part of the thighs, and arms; showing the slightly to moderately
scaly macular and circinate patches—in some places confluent.
and young adults, less frequently in those of dark hair and complexion
than in those of the medium and blonde types.1 The essential cause is
1 Towle, Jour. Cutan. Dis., April, 1904, from an analysis of 202 cases—158 from the
records of the dermatologic department of the Massachusetts General Hospital, and 44
from the private records of Dr. John T. Bowen—states: Pityriasis rosea occurs in the
two forms—the macular and the circinate—with about equal frequency; affects most
often the trunk and upper part of the extremities, but is occasionally limited to one
part; it is more frequent in the autumn months, and by far more common in women
than in men; recurrences, though rare, do occur; race and occupation have no influence.
His other conclusions are about the same as outlined in the text; D. W. Montgomery,
ibid., 1906, p. 167, gives a clinical analysis of 38 cases.
PITYRIASIS ROSEA
197
unknown, but that time will disclose a parasitic factor is scarcely to be
doubted. According to Thibiérge, the disease does not recur, but this,
I believe, does occasionally take place. There is a growing tendency,
not without reason, to consider the disease as possessing contagious
properties of, however, a feeble character; 2 cases in the same family
have been observed by Crocker,1 Zeisler,2 Fordyce,3 and G. H. Fox.4
Pathology.—Many of the European dermatologists, especially
those of Austria, have looked upon this disease as disseminated ring
worm, called by them herpes tonsurans maculosus; but English, French,
and Americans are well assured of the individuality of the disease, in
which ringworm fungus is never found. The truth of the matter seems
to be that there is a disseminated ringworm, infrequent, it is true, but
seen chiefly in Austria, which closely resembles it, although many of the
cases so considered are doubtless those of pityriasis rosea.
While pityriasis rosea is probably of parasitic origin, as yet no one,
excepting Vidal,5 whose findings have never been corroborated, except
possibly recently by Du Bois,6 has ever discovered a parasite. Other
views held as to the nature of the disease are: that it is allied to derma
titis seborrhoica, and that it may be a mildly inflammatory disease,
somewhat similar to psoriasis. There is, it is true, in some cases a close
clinical resemblance to the seborrheic disease, which was pointed out
by Besnier,7 and in my experience it is sometimes so close as to lead to the
belief that it may possibly belong under that head.
The pathologic anatomy of this disease has been investigated by
Jacquet, Unna, Tandler, and Towle, and, upon the whole, indicates that
the process in the earlier stage or in mild cases is an extremely mild
inflammation seated in the upper cutis, of a serous and hyperplastic
character, always more marked toward the periphery; in the later
stages or in more pronounced lesions the inflammatory changes are
emphasized, and there is displayed a tendency to irregularly formed
minute pressure vesicles beneath the corneous layer, but which are
not macroscopically visible. Almost the whole papillary body is con
verted into a net of spindle-cells with stellate connecting processes.
Diagnosis.—The disease is to be distinguished from dermatitis
seborrhoica, tinea circinata, psoriasis, and the maculopapular scaly
syphiloderm.
1 Crocker, Diseases of the Skin, second ed., p. 288 (2 instances in 2 members of the
same family).
2 Zeisler, Jour. Cutan. Dis., 1893, p. 494 (husband and wife).
3 Fordyce. ibid., p. 497 (husband and wife), and ibid., 1898 (Soc'y Trans.), p. 340
(in 2 sisters occupying same room).
4 G. H. Fox, ibid, (mother and child).
5 Vidal, Annales, 1882, p. 22.
6 Du Bois, Annales, Jan., 1912, p. 33, claims to have found a fungus closely resembling
the microsporon described by Vidal, appearing as masses of round spores of variable
size and no mycelia, and proposes the name, in honor of Vidal, of “microsporon dispar.”
The spores were found within the follicular and glandular orifices. Du Bois describes
3 cases exemplifying what he calls three types of the disease—the pityriasis rosea of
Gibert, the common type, and two other rarer varieties, a psoriaform parakeratosis
and the type described by Vidal as pityriasis circiné et marginé. The fungus was
found in all.
7 Besnier, Annales, 1889, p. 108; D. W. Montgomery, Jour. Cutan. Dis., 1906, p.
167, discusses this as well as other points in an analytical paper (38 cases).
198
INFLAMMATIONS
Seborrhea differs in having greasy scales, in its more gradual appear
ance, in its usually taking its start from a seborrhea of the scalp or
eyebrows, and in the evolution and character of the patches and its
persistent course. Seborrheic patches sometimes show (over the ster
num) slight projection into the sebaceous follicles; in some cases the diag
nosis may be difficult at first, but a short observation will usually suffice
to clear up any doubt.
Ringworm is rarely seen in such profusion as pityriasis rosea, the
ring shape is more distinct, there is a more decided disposition to central
clearing, even when the patches are small; the peripheral portion is
usually more sharply marginate and occasionally is vesicopapular or
vesicular. Typical ringworm patches are also often seen about the face
and hands, unusual sites for pityriasis rosea. In suspected cases scrap
ings from the peripheral portion should be examined by the microscope
(see Ringworm).
Psoriasis is, as a rule, more inflammatory, the periphery more sharply
marginate, the scaling more profuse, and patches are also frequently
seen in the scalp, especially toward the border of the forehead and mas-
toid regions, and generally to be found likewise on the extensor surfaces
of the knees and elbows. It usually comes on slowly, and at first rarely
displays any tendency to ring-formation.
The maculopapular syphiloderm, if scaly, bears a close resemblance,
but there is usually distinct infiltration, it is of a darker color, and lesions
are not unusual on the palms and face; as it is an eruption of the active
stage of syphilis, one or more corroborative symptoms are always to be
found.
Prognosis and Treatment—The disease usually runs its course
in three or four weeks to a few months, disappearing spontaneously.
As a rule, there is no special tendency to recurrence. It has seemed to
me that the use of certain external applications tends to shorten its
course, such as a mild sulphur ointment, from 20 to 60 grains (1.3 to 4.)
to the ounce (32.) of petrolatum or benzoated lard, or one containing
from 10 to 30 grains (0.65 to 2.) of salicylic acid; or an ointment contain
ing both of these ingredients may be prescribed:
R. Acid, salicylici, gr. xv (1.);
Sulphur, præcip., gr. xxx (2.);
Petrolati,
Ungt. aquæ rosæ, ââ 3ss (16.).
The selected ointment is to be gently rubbed in, in small quantity,
once daily; the excess wiped off, and a mild dusting-powder applied.
The application is to be preceded every day or every other day by an
ordinary soap-and-water bath; or, in cases in which the scaliness is
somewhat more abundant than usually observed, with an alkaline bath.
Lotions applied with a piece of lint or as a spray can be employed in
place of the ointments, but do not seem to exercise as much influence,
althought they are more agreeable, and have more effect in control
ling the itching if present; the following may be used: Carbolic acid,
1½ drams (6.) to the pint (500.) of water, to which a dram (4.) of gly-
DERMATITIS EXFOLIATIVA I99
cerin and an ounce (32.) of alcohol may be added; and a lotion of boric
acid, 15 grains (1.) to the ounce (32.) of water, with also from 5 to 10
grains (0.32 to 0.65) of resorcin added. In addition to the external
applications a saline laxative may be occasionally prescribed, along with,
if in any way indicated, such tonics as quinin, strychnin, and iron.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |