| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
THE CHRONIC RESISTANT MACULAR, AND MACULO-PAPULAR SCALY ERYTHRODERMIAS
The various cases considered under this head seem sufficiently dis
tinctive to separate them from the various dermatoses to which they
bear resemblance. They have all much in common and, according
as the one or other feature is the more pronounced, are, in some of their
clinical aspects, suggestive of seborrheic eczema, sometimes of seborrheic
eczema of a moderately to markedly psoriatic type, of pityriasis rosea, of
the early prodromal erythematosquamous eruption of granuloma fun-
goides, and the disappearing and almost disappeared plaques of lichen
planus. They have been grouped by Brocq under the head of para-
psoriasis; by Crocker, under lichen variegatus; by Jadassohn, under
psoriasiform and lichenoid exanthem, and dermatoses psoriasiformes;
and by Colcott Fox and Macleod, under resistant maculopapular scaly
erythrodermias. Of the 4 or 5 cases that I have met with in the
past several years, a few were closely simulative, clinically, of a mild
seborrheic eczema, with some features of a pityriasis rosea, and a few,
in their general aspects, represented, clinically, a medley of a mild sebor-
rheic eczema and a disappearing lichen planus, the whole having a varie
gated or marbled appearance.
The first cases of importance were reported under the name para-
keratosis variegata, by Unna,1 in collaboration with Santi and Pollitzer.
They were characterized by a more or less generalized red exanthem, but
sparing the head, palms, and soles, leaving in some regions—trunk and
thighs—small irregular sunken patches of normal skin free, giving the
eruption a reticulated or mottled appearance. Over the reddened por
tion there was a fine lamellar desquamation. The color was deeper
on the lower portion of the body, but not uniform, even for the same
region, varying from a yellowish red to a bluish red. The affected patches
were slightly raised from the surface, their borders sharp, their cuticular
areas slightly marked, and their surface beneath the desquamating scales
bright and waxy. The larger patches appeared to the touch decidedly
infiltrated, like an erythema papulatum, the smaller patches resembling
1 Unna, Santi, and Pollitzer, Monatshefte, 1890, vol. x, p. 404; abstract in Brit.
Jour. Derm., 1890, p. 217.
SCALY ERYTHRODERMIAS 225
recent lichen planus papules. There were no subjective symptoms. The
affection had lasted in both cases for several years or longer. One of
the cases had been sent to Hamburg by Besnier, who had at first regarded
the disease as an unusual form of lichen planus universalis, but con
cluded, after a time, that the affection was one sui generis. The histo-
logic examination showed in both cases the changes to be limited to the
papillary layer and the epidermis.
In both cases the malady proved resistant to the most energetic
chrysarobin treatment, and yielded only to a vigorous course of applica
tions of pyrogallol, during which treatment the poisonous effects of this
drug from absorption were prevented by the exhibition internally of large
doses of dilute hydrochloric acid.
Under the name erythrodermie pityriasique en plaques disseminées
Brocq1 recorded a case of a superficial patchy, slightly scaly eruption,
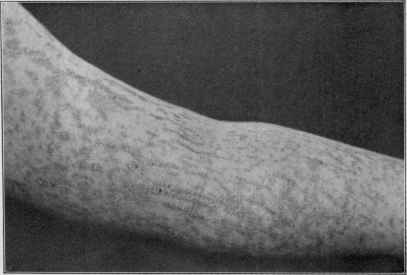
Fig. 44.—Parakeratosis variegata.
which he was inclined to believe had some features in common with
parakeratosis variegata, just referred to, a conclusion with which J. C.
White2 does not agree, a material and essential difference being the
1 Brocq. Journal des praticiéns, 1897, p. 577; and “Parapsoriasis,” Jour. Cutan. Dis.,
1903, p. 315 (with review and references).
2J. C. White, Jour. Cutan. Dis., 1900, p. 536 (with histologic examination by
C. J. White); Colcott Fox and Macleod in a recent valuable and exhaustive clinical
and histologic contribution, “On a Case of Parakeratosis Variegata,” Jour. Cutan. Dis.,
1901, p. 424, and Brit. Jour. Derm., 1901, p. 319, go over the entire literature of cases
which seem to present similar or allied conditions; Méneau, Jour. mal. cutan., May,
1902 (parakeratosis variegata; man aged twenty-one; had existed since aged ten);
Graham Little, Brit. Jour. Derm., 1902, p. 218 (erythrodermie pityriasique, case
demonstration; girl aged ten); C. J. White, Jour. Cutan. Dis., 1903, p. 153 (1 case,
with histologic illustration); Anthony, Jour. Cutan. Dis., 1906, p. 455 (1 case, clinical
and histologic, with brief review and bibliography); Török in Mrâcek‘s Handbuch;
Riecke, Archiv, 1907, vol. lxxxiii, pp. 51, 205, and 411 (3 cases, lichenoid, with analytic
15
226 INFLAMMATIONS
entire absence of any papular tendency. The eruption is characterized
by scattered, variously sized, scarcely elevated plaques, which are
fairly well or quite sharply defined; are of a brownish, pale-rosy, or
pale-red color, and with a surface very slightly scaly, the scaliness
varying considerably, being extremely slight in White‘s first case,
somewhat more pronounced in his second and third cases, as well as
in Brocq‘s patient, but never excessive or conspicuous. The brownish
tint is sometimes the predominant shade, although in Brocq's patient
a tawny hue was more noticeable; for the most part, however, the color
is pale red or rosy. There is often an ill-defined, marbled, and reticu
lated appearance of the eruption. The eruption is more or less general,
the trunk especially being favored, and sometimes the patches coalesce
in places. It is at its worst in winter, and partly or wholly disappears in
mild weather. The eruption, as a rule, gives rise to no troublesome sub
jective symptoms; occasionally there is slight itchiness. The integu
ment is rather dry, the perspiratory function seeming to be lessened.1
Of the cases reported, one was in a child aged nine, the others were adults,
Brocq‘s case being advanced in years. In another instance in a case
recently reported by Ravogli,2 which, he considers, possesses features
which place it with the cases just referred to, the patient was aged three,
and the eruption almost universal, but still showing the coalescence
from rounded patches of considerable size. This patient had had two
previous attacks.
Brocq, in a later paper, divides the cases—under the name of para
psoriasis—into three groups: (I) Parapsoriasis guttata (bearing close
relationship or resemblance to psoriasis); (2) parapsoriasis lichenoides
(intermediate in relationship or resemblance between lichen and psoriasis);
(3) parapsoriasis in patches (closely allied and showing resemblance to
seborrhœa psoriasiformis (dermatitis seborrhoica), the érythrodermies
pityriasiques en plaques disseminées). These cases are characterized
by (1) an almost complete absence of pruritus; (2) a very slow evolution;
(3) a distribution in circumscribed, sharply defined patches, whose dimen
sions are from 2 to 6 cm. in diameter, which are scattered here and there
over the integument; (4) an almost complete absence of infiltration of the
derma; (5) a pale redness (pinkish colored); (6) a fine pityriasic desqua-
mation; (7) an extraordinary resistance to the local applications usually
review of reported cases); Trimble, “The Chronic Scaly Erythrodermias” (3 cases,
with cuts and brief review and references), Jour. Amer. Med. Assoc, 1909, vol. liii, p.
264; Corlett and Schultz, Jour. Cutan. Dis., 1909, p. 49 (3 cases with review, references,
and histologic plates); Morris and Dore, Brit. Jour. Derm., 1910, p. 249, 1 case,
lichenoid type (parakeratosis variegata), in man aged fifty, of six to eight years’ dura
tion; good illustration; Arndt (Lesser‘s Clinic), Archiv, Bd. c, Heft 1-3 (8 cases,
with review, histologic cuts, and bibliography); Hodara, Dermatolog. Wochenschr.,
July 6 and 13, 1912, vol. 1v, pp. 848 and 877, a case of parakeratosis variegata (Unna‘s
type); review, bibliography, and histologic cut; Wilfred Fox, Brit. Jour. Derm., 1912,
p. 21—case demonstration; patient, woman aged forty-nine; pityriasis lichenoides
chronica or lichen variegatus type; began on face, and now (five years later) has ex
tended downward to middle of trunk, with patches on buttocks and thighs; past year
few isolated bullæ have been appearing, particularly on the neck and shoulders.
1 In Trimble‘s 3 cases there was a very noticeable and rather excessive sweating on
the face, which, as is usually the fact, was not involved in the disease.
2 Ravogli, Jour. Amer. Med. Assoc, July 13, 1901 (with histologic examination by
Heidingsfeld).
LICHEN SCROFULOSUS
227
employed in the treatment of psoriasiform or pityriasic seborrhea; in
fact, only yielding slowly and imperfectly to the most energetic appli
cations of pyrogallol.
The pathologic histology has been studied by Brocq, Colcott Fox
and Macleod, C. J. White, and others. C. J. White found, both in
J. C. White's case and his own, the following: (1) Open network forma
tion of the stratum corneum, composed of non-nucleated horny cells;
(2) absence of the stratum lucidum; (3) great atrophy, or even total
absence, of the stratum granulosum; (4) in places, compression of the
rete cells and reduction of the layers composing the stratum spinosum;
absence of the palisade layer; and, finally, greatest divergence from the
normal directly over the parts of the corium mostly affected; (5) edema-
tous condition of the corium; and (6) reduction in the amount of elastin.
Macleod's study1 of the Colcott Fox-Macleod case and of Perry's case
(about the same type as the White cases) showed: Dilatation of the
subepidermal capillaries; a flattening and edema of the papillary body; an
attenuation of the fibrous element; an infiltration of small cells, consisting
of small connective tissue cells, mast-cells, and leukocytes; a thinning of
the epidermis; an edema and dilatation of the nuclear spaces; a deficiency
in the transitional layers, and an imperfect stratum corneum. Corlett
and Schultz‘s findings are in a measure similar, but they indicate also,
as partly foreshadowed by C. J. White, that there is primarily a basic
vascular involvement to which the other cutaneous changes are due,
beginning as an endothelial hypertrophy and hyperplasia, with con
secutive perivascular infiltration and proliferation, leading to narrow
ing and complete obliteration of the lumina of the veins; the arterioles
may show endothelial swelling, but this occurring only after the peri-
phlebitis is well marked.
The treatment of these cases, as already referred to, is not very satis
factory. Engman2 and Mook report improvement with the administra
tion of mercuric chlorid, believing its favorable effect due to its action
on the thickening of the vessels. The local remedies most efficacious
seem to be those commonly employed in psoriasis, especially pyrogalIol.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |