| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
VACCINAL ERUPTIONS
Synonym.—Vaccination rashes.
It is beyond the scope of this volume to go into the method and
details of vaccination more than briefly, and chiefly as to the cutaneous
aspect of the resulting lesions, and the sometimes engendered or pro
voked more or less generalized eruptions. Vaccinia, or cow-pox, is a
well-known affection among certain animals, but more especially the
cow, and while never occurring spontaneously in the human subject,
its artificial production in the latter by inoculation, as strenuously pointed
out by Jenner, affords a protection against variola.
The operation of vaccination is sufficiently well known to need no
comment.1 For the first few days nothing special is observed: possibly
a little congestion or irritation from the procedure. After the lapse of
forty-eight hours or thereabouts a minute papule is noticed at the point
or points of inoculation, which in the course of two or three days more
has developed into a vesicle. Where several or more have simultaneously
arisen at contiguous points of the inoculation spot these usually merge,
and the subsequent course is, as a rule, the same as when there is but
one inoculation point, although in some instances the resulting larger
vesicle shows its compound nature. When several inoculation points
are, as the result of intention or accident, at some distance apart, each
develops and usually goes through the regulation course, although some
times one undergoes full development and the others partial. The vesicle
enlarges peripherally, and in from five to seven days after the operation
is a somewhat distended, well-formed pea- to finger-nail-sized, translu
cent vesicle, frequently with a perceptible or well-marked tendency to
central depression or umbilication. At this stage, in successful, and
usually especially pronounced in instances of first vaccination, there is
a well-defined wide encircling red or pinkish-red areola, with some
inflammatory infiltration or hardness. At this time—in the sixth to the
eighth day—constitutional symptoms of variable degree present: slight
temperature elevation, accelerated pulse, general malaise, often some
gastrointestinal uneasiness, and the axillary or neighboring lymphatic
glands are somewhat enlarged and tender. The lesion is usually ex
quisitely sensitive, and slight or intense itchiness may, at this time, be
1 Hutchins, Jour. Amer. Med. Assoc, April 23, 1898, advises a simple, ingenious,
painless method, especially valuable in children, in whom even the suggestion of a
trifling scarification often meets with opposition. The part to be vaccinated is first
cleansed, and a small piece of cotton is wet with liquor potassæ and laid on the spot for
two or three minutes; it is then removed, and the soapy mixture thus formed, with the
epidermis and skin secretion, wiped off, and the place gently rubbed with a piece of
damp cotton; the epidermis, softened by the liquor potassæ, comes readily away, and an
excellent bloodless absorbent spot is thus made, on which the vaccine is placed and let
dry on in the usual way.
VACCINAL ERUPTIONS
487
complained of. The vesicular contents now become cloudy, and by
the ninth or tenth day desiccation gradually sets in, the inflammatory
areola begins to fade, and the general symptoms subside, the lesion then
finally, by the thirteenth to the fifteenth day, presenting as a dime- to
silver-quarter-sized yellowish or reddish-brown crust, with an encircling
narrow line of redness, which latter slowly disappears; and usually in
a little less than three weeks from the date of vaccination the crust has
fallen off, disclosing a pinkish or reddish scar which slowly becomes
whitish and shows minute pits or depressions—the sites of the primary
points of inoculation. Exceptionally, generally in those cases in which
healing has been accidentally delayed, a keloidal tendency has been
noted, but usually of slight development.
All cases are not regular in their development and course: in some
the vesicle develops early, in others it is retarded. Cases vary con
siderably in intensity, in some, probably from accidental complication
or inoculation or individual peculiarity of the tissues, the zone of red
ness presents a decidedly erysipelatous aspect, and may involve a greater
part of or the entire region. In fact, so severe may this erysipelatous-
looking inflammation be that it may assume a phlegmonous character
and some sloughing of the vaccinated spot occur, with associated lym
phangitis and marked swelling of the neighboring glands. The con
stitutional symptoms may also be correspondingly severe. In other
instances new vaccinal lesions develop in the neighborhood of the vac
cinated spot, and even to some extent beyond, and while these may be
simply a part of the disease vaccinia, it is much more probable that they
are the result of accidental inoculation in consequence of carrying the
virus from the vaccine lesion by means of the nails or fingers. General
vaccinia has, however, it is stated, been observed, although the possi
bility of a coincident impetigo contagiosa might afford an explanation
of many such instances. In some cases of vaccination, usually unsuc
cessful, after a partial formation of the vaccine vesicle, it is ruptured,
and granulation tissue of a raspberry- or strawberry-like character de
velops, and sometimes, if untreated, will persist for weeks without show
ing the slightest tendency to spontaneous disappearance; in some of its
aspects presenting a resemblance to granuloma pyogenicum. In some
such instances there has apparently been aft accidental, but usually harm
less, inoculation of an adventitious organism or material, and which prob
ably has taken place subsequently to the vaccine inoculation. It may
be that in some of these cases the tubercle bacillus is implanted upon
an unfavorable soil and fails to gain proper nutritional support, and dis
appears on the institution of almost any astringent or antiseptic applica
tion.
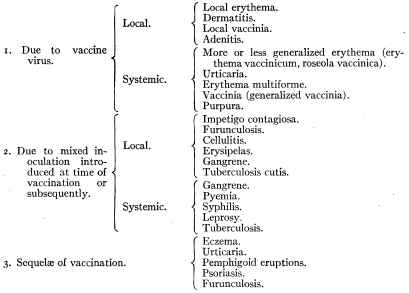
Malcolm Morris, in his excellent presentation of the subject, has
divided the vaccinal rashes1 into two classes: (1) Eruptions due to pure
1 The reader desirous of pursuing the subject is referred to Behrend‘s paper (read
before Dermatologic Section of International Medical Congress, London, Aug., 1881),
Arch. Derm., 1881, p. 383 (translated by Alexander); Morrow, Jour. Cutan. Dis.,
1883, p. 166, with references; Malcolm Morris’ paper, with discussion (read before
Dermatologic Section, British Medical Association, Birmingham, Eng., July, 1890),
Brit. Med. Jour., Nov. 29, 1890—abstract of paper in Brit. Jour. Derm., 1891, p. 26;
488 INFLAMMATIONS
vaccine inoculation, and (2) eruptions due to mixed inoculation, which
Frank has slightly enlarged and modified, and which, with few immaterial
changes, embody my own views and present clearly the eruptive com
plications: some not uncommon, others extremely rare, and some ques
tionable. It is true that to some extent these divisions are more or less
arbitrary, and there is difficulty in placing some affections as respects
the exact etiologic local or general relationship, and hard-and-fast lines
cannot always be drawn; but the scheme is about as satisfactory as can
be made under present conditions, and gives a faily clear presentation of
the subject.
The most frequent and usually evanescent and harmless of these
are the localized or general erythema, urticaria, erythema multiforme, a
regional, vaccinia-like eruption (often probably impetigo contagiosa),
impetigo contagiosa, and a pseudo-erysipelatous or erysipelatous in
flammation, or other accidental dermatitis. A neighboring adenitis,
as already referred to, is usual to a moderate degree, but sometimes is
extremely developed. Local or generalized erythema, erythema multi-
forme, and urticaria may present at any time between the date of vac
cination and the crusting period; erythema multiforme and urticaria,
especially the latter, even to a later period. Behrend called attention
to the fact that there seem to be two periods for the occurrence of vac-
cinal eruptions—in the first three days, or not until the eighth or ninth.
While true in the main, there are many exceptions. They present no
also Frank‘s paper, Jour. Cutan. Dis., 1895, p. 142; and Dyer‘s, New Orleans Med.
and Surg. Jour., Feb., 1896; Colcott Fox, Brit. Med. Jour., July 5, 1902; Towle, Boston
Med. and Surg. Jour., Sept. 4, 1902; Stelwagon, Jour. Amer. Med. Assoc., Nov. 22,
1902; Pernet, Lancet, Jan. 10, 1903; Corlett, Jour. Cutan. Dis., 1904, p. 495 (with
illustrations and references to recent papers). See also under Pemphigus and Derma
titis herpetiformis.
VACCINAL ERUPTIONS
489
special peculiarities from the ordinary types of these maladies, but are
usually of shorter duration. In erythema multiforme the erythematous
and erythematopapular manifestations are most common, but the vesic
ular and bullous lesions may also occur. The various other cutaneous
complications are rare. Eczema developing from the inoculation site
or elsewhere occasionally follows, but probably only in those with a clear
eczematous tendency; and exceptionally the disappearance of an existing
chronic eczema is promoted by the vaccinal operation (see Eczema).1
Psoriasis has in rare instances taken its start at the point of inoculation,
or has made its first appearance closely following this procedure, as
already referred to under that disease; in all probability vaccination
has no etiologic relationship except as possibly its action as a local or
general excitant or its disturbing influence upon the nervous system.
Indeed, in this as in many other instances of eruption occurring during
or immediately subsequent to vaccination it is more than probable that
they are purely coincidental and in no way connected with or due to
this operation. The layman and, flagrantly, the antivaccinationist,
and sometimes, too, the physician, are too prone to consider all such
eruptions as effects; in short, it should be clearly understood that cuta
neous outbreaks occurring at such time are not necessarily vaccinal,
although it is true many of them are.
Most of the pemphigoid eruptions encountered, usually following
one to several weeks after the operation, have doubtless been examples
of bullous impetigo contagiosa. Exceptionally, however, pemphigus
or pemphigoid lesions have been observed.2 A few instances of seeming
relationship have come to my notice, and of serious character; bovine
virus was used. In this connection the observations and study of the
etiology of acute pemphigus by Pernet and Bulloch3 are of great interest
(see Pemphigus). In their report and analysis of cases, in a number the
subjects were found to be butchers, and the disease to have originated
from a small wound resulting from their occupation; further, in one case
a pemphigoid eruption seemingly followed inoculation from a similar
eruption on the teats of a cow. Others are also mentioned where the
disease occurred in those having to do with animals or animal products,
and instances of the existence of pemphigoid eruptions in animals are
referred to. These facts have suggested the possibility that the rare
cases of pemphigus, usually of grave character, exceptionally observed
developing after vaccination, may thus be explained.
Irrespective of the usual transitory rashes, it has been believed,
1 Great care should be exercised, however, as to vaccination in moist, raw, oozing
cases of eczema; as in a few instances, in young children, more or less general inocu
lation of such surfaces has followed. One such case was shown at the Internat. Derm.
Congress in Berlin, Sept., 1904.
2 See a recent interesting paper by Bowen, “Six Cases of Bullous Dermatitis Follow
ing Vaccination, and Resembling Dermatitis Herpetiformis,” Jour. Cutan. Dis., 1901,
p. 401; and Howe, “Cases of Bullous Dermatitis Following Vaccination,” ibid., 1903,
p. 254. Other references will be found under Dermatitis herpetiformis.
3 Pernet and Bulloch. Brit. Jour. Derm., 1896, pp. 157 and 205. See also Bowen's
suggestive paper, “Acute Infectious Pemphigus in a Butcher, during an Epizoötic of
Foot and Mouth Disease, with a Consideration of the Possible Relationship of the
Two Affections,” Jour. Cutan. Dis., 1904, p. 253; also “Report of Bureau of Animal In
dustry,” abstract, Jour. Amer. Med. Assoc, 1909, vol. lii, p. 1679.
490
INFLAMMATIONS
ever since the operation of vaccination has been advocated, that the
process is not without danger as to the inoculation of other more serious
diseases. There can be no question that pure virus of bovine origin
should be employed, and that with this, as with any operative procedure,
care, caution, and cleanliness are essential prerequisites to safety, and
with proper observance of which the operation is an absolutely harmless
and safe one. With careless operators impure virus, and more especially
uncleanly patients, the accidental inoculation of tuberculosis, leprosy,
syphilis, and other affections becomes a possibility. It is doubtless true
that in most of the serious sequences of vaccination that neither the
operator nor virus is at fault, but that the damaging infection takes
place later as a result of carelessness, negligence, or uncleanliness on the
part of those vaccinated. The possibility of inoculation of tuberculosis
has been questioned, but suggestive cases are on record where localized
tuberculosis cutis (q. v.) has developed at the point of vaccination, and
that much being admitted, general infection might likewise be produced.1
As to the accidental inoculation of leprosy, there has long been a belief
that such has often occurred (Beaven Rake), but authentic examples
are rare. Daubler's2 2 cases seem to show this possibility, and doubtless
other instances might be found upon investigation. Added to this is
the fact that bacilli lepræ have been found in the vaccine lymph taken
from a leper (Arning).3 Examples of syphilis inoculation through vac
cination are rarely observed at the present day, and then only
through gross carelessness or through pure accident unconnected with
the procedure itself; but that it was, while not frequent, occasionally
observed formerly is attested by the observations of Hutchinson, Four-
nier, R. W. Taylor, and others.
Vaccinal eruptions cannot always be prevented, referring especially
to those that arise through the vaccine virus itself, but such are prac
tically harmless and short-lived, and rarely give rise to trouble. Even
taking into consideration the occasional accidental mixed infections,
which also with rare exceptions are not of serious import, such cases
weigh as nothing compared to the benefit bestowed upon mankind by
the operation. With proper care, however, on the part of the caretakers
of the cattle from which the virus is derived, rigorous inspection of the
animals, and extreme precaution in the collection and preservation of
the vaccine, added to caution and cleanliness on the part of physician
1A case under my own observation, of development of lupus at the site of vaccina
tion, and immediately following the same, and which is referred to in discussing that
disease, is one in point. This patient and two others were vaccinated from the same
crust; the reactionary symptoms in all were severe, in two quickly followed by mixed
general symptoms of what seemed, as described to me, of mixed septicemic and tuber
culous character, followed by death; and in my patient, at that time a robust young
female child, followed by the development of lupus, which had persisted and extended
when I saw her ten or twelve years later. The history of the cases was given me by a
physician, the brother of my patient, but owing to the years which had elapsed and the
nature of the accident, further details could not be obtained, and there naturally
remains an element of doubt about the true character of the condition which carried
off the other patients.
2 Daubler, “Ueber Lepra und deren Kontagiosität,” Monatshefte, Feb. 1, 1889,
p. 123.
3 Arning, Jour. Lepr. Inves. Com., No. 2, Feb., 1891, p. 131, quoted by Dyer
(loc. cit.).
VACCINAL ERUPTIONS 491
and patient, before, at the time, and subsequently to the operation until
complete healing has taken place, the occurrence of serious accidents
would practically be placed beyond the bounds of possibility. Human
virus should, of course, never be employed. Morris, among other rec
ommendations for the prevention of vaccinal eruptions and accidents,
urges that strict antiseptic and protective treatment should be carried
out immediately after the vesicles have developed, and, further, that
the cases should be seen by the vaccinator until the wounds have healed.
But little need be said about the treatment of the various erythem-
atous, urticarial, and other ordinary rashes occasionally observed, as
it is in these the same as in these eruptions occurring independently
of the operation. The rare serious cases, too, are likewise managed on
the same principles laid down elsewhere for the particular eruption
presenting.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |