| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
X-RAY DERMATITIS
Synonyms.— X-ray burn; Röntgen-ray dermatitis or burn.
The “Röntgen ray” discovery has added much to the resources of
medicine, especially in a diagnostic way, and to some extent therapeu-
tically, but as now known it is
not the harmless agent it was
at first thought.
Its deleterious effects upon
the integument, and sometimes
subcutaneous tissues, and excep
tionally extending to the bone,
are now matters of record, and
have led to its more careful
employment, although in spite
of all precautions, probably from
some extreme susceptibility of
the skin in certain subjects, an
occasional case of cutaneous in
jury still continues to be reported
from time to time.
The first signs of cutaneous
disturbance sometimes do not
present for several days or longer
after exposure. The mildest
phase of the x-ray action is a
peculiar reddish flush or ery
thema, resembling somewhat
closely sunburn, and which in
the course of several days or a
few weeks gradually disappears.
In other instances of seemingly
similar mild type the flush con
tinues for a longer period, and
not infrequently there is an ex
tremely slight feeling of local dis
comfort, such as a sensation of
warmth, burning, or itching. A
continuance of exposures, and
occasionally after only a few exposures, this flush is succeeded by a varying
number of brown to black freckles, and a slight general pigmentation of
the skin. These conditions may persist for several weeks, and in extreme
cases much longer; exceptionally an insignificant growth of down and
telangiectases are added. On the other hand, accidental exposure of
a hairy region will exceptionally, even though of comparatively short

Fig. 108.—The hand of an x-ray opera
tor, showing the atrophic condition of the
nails and skin; the latter is dry, slightly
scaly, with pigmentation, thinning, and
wrinkling.
X-RA Y DERMATITIS
445
duration, cause falling of the hair—followed, sooner or later, by regrowth.
In other cases the erythema is rapidly succeeded by a superficial, ill-
defined vesiculation, and with or without an associated trifling swelling
or puffiness. These are usually much more persistent, and may be
attended with the ordinary subjective symptoms of irritation. In
some instances a slight dry branny or insignificant, sometimes lamellar,
scaliness or exfoliation follows the erythema, appearing several days or
later, or first showing itself as the redness is fading away. In those
whose hands are constantly exposed to the ray, as with those making
frequent use of it professionally, a mild erythematosquamous condition
of these parts not infrequently develops, and is more or less persistent,
and is succeeded by variable pigmentation, wrinkling and other atrophic
changes in the skin. Brittleness and thinning of the nails are also often
noted. When such exposures have been long continued these changes
persist for several months to several years, or more, after the operator
has given up x-ray work; in fact, in some instances the hands never fully
recover their normal condition, and in a few cases keratoses are super-
added, which may develop into carcinoma.1 The possibility of these
atrophic changes are to be kept in mind in the employment of x-ray
treatment for the benign dermatoses, such as acne, for in a few instances
a thinning, atrophic, and freckle, or other pigmentary and old-age changes
(wrinkling, atrophic spots, telangiectases, etc.)2 have been noted. Two
such cases have come under my own observation.
A far more serious state of affairs is occasionally, but fortunately
infrequently, noted, in which the erythematous flush, sometimes with
subsequent vesicular development, is followed by a dry, leathery, super
ficial or deep slough or ulcer. The ulcer is, as a rule, shallow, sluggish-
looking, with a slightly or moderately hyperemic or inflammatory border,
and covered with a rather adherent grayish, often tough and leathery
crust or membrane; it is persistent, with but little if any tendency to
spontaneous reparative change, and the accompanying pain is often
excruciating, as in cases observed by Orleman,3 Cassidy,4 and others.
Etiology and Pathology.—There is much divergence of opinion
as to the exact etiologic factor in the production of x-ray burns. Gil-
christ5 and others have suggested that it might be due to the entrance
of minute particles of the conducting metal used; others (Leonard,6
Johnston, Phila. Med. Jour., Feb. 1, 1902; Macleod (Brit. Jour. Derm., 1906,
p. 104), reports an epithelioma developing on an x-ray scar in a case of lupus vulgaris;
Bunch, “ X-Ray Dermatitis and Epithelioma,” Brit. Jour. Derm., 1910, p. 339, reports
a somewhat similar case, and the tendency to epitheliomatous changes in the keratoses
consequent upon x-ray dermatitis. That this latter may be finally serious is evidenced
by several or more reported deaths. A late example of this was Dr. Kesabian, a wrell-
known radiographer, of Philadelphia, epitheliomatous changes starting in the hand
keratoses, and in spite of hand amputation, finally involving the axillary glands, and
other parts.
2 Freund and Oppenheim, “Uber bleibende Hautveränderungen nach Röntgen Ver-
strahlung,” Wien. klin. Wochenschr., 1904, No. 12.
3 Orleman, Wien. med. Wochenschr., 1899, No. 39.
4 Cassidy, Med. Record, Feb. 3, 1900 (with illustrations).
5 Gilchrist, Johns Hopkins Hosp. Bull., Feb., 1897 (with an illustration and review
of published cases, with bibliography).
6 Leonard, New York Med. Jour., July 2, 1898.
446 INFLAMMATIONS
Oudin, Barthélemy and Darier,1 and others) that the current, and not
the rays, is responsible; the latter believing, as now generally accepted,
that too short a distance of the tube and a current of high intensity are
the dangerous factors. Tuttle2 suggested that the exposure to the
x-ray generated by the static machine was apparently not productive
of injury, but this is refuted by Cassidy‘s extreme case (loc. cit.) and
probably by others. The light-ray itself does not seem to me to have
been given full consideration as the possible causative or influencing
factor. The pathology of the malady is not clearly understood, although
many observers believe that the cutaneous disturbances are not primary,
ascribable to local action on the cells of the derma, but that they are
rather of a trophoneurotic nature, due to neuritis; and this, according to
Oudin, Barthélemy, and Darier (loc. cit), is not a peripheral neuritis
connected with the dermic nerve terminals, but is probably at first central,
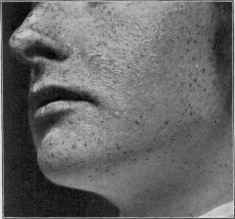
Fig. 109.—X-ray dermatitis of mild degree, showing an erythematosquamous condi
tion, and also diffused and freckle-like pigmentation (case of acne—cured—skin regained
its normal state in several weeks).
during the period which might be called that of the incubation of the
phenomena, to become subsequently centrifugal and to manifest itself
by distinct alterations of nutrition.3 Behrend4 is of the opinion that
the integumentary changes—scaliness, vesiculation, falling of the nails
and hair—are due to the serous exudation induced in the cutaneous
tissue.
Macleod,5 after reviewing the investigations of others, gives the fol-
1 Oudin, Barthélemy and Darier, La France Medicate, 1898, No. 12 (a valuable
conjoint paper, based upon its use in 400 cases, detailing the various accidents and dis
cussing the pathology); Zarubin, Monatshefle, 1899, vol. xxviii, p. 489, also gives a
valuable résumé and bibliography.
2 Tuttle, Soc‘s Trans., Philada. Med. Jour., Feb. 26, 1898.
3 Quoted from review of the subject in Progressive Medicine, Sept., 1899.
4 Behrend, Berlin, kiln. Wochenschr., June 6, 1898.
5Macleod, Brit. Jour. Derm., 1903, p. 365 (with brief review and reference to the
works of Oudin, Barthélemy and Darier, Schiff, Freund, Doutrelepont, Beck, Pernet,
Scholtz, Skinner, Norman Walker and Gardiner, and others).
X-RAY DERMATITIS 447
lowing tentative propositions as fairly representative of the present state
of our knowledge of the subject: (a) That the x-rays in small doses have
a stimulating effect on the elements of the healthy skin; (b) that in large
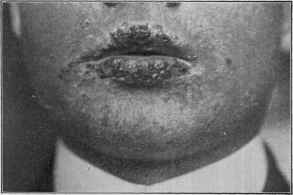
Fig. no.—X-ray dermatitis of considerable severity; shows the importance of protect
ing the lips in sensitive subjects, or when the exposure is somewhat prolonged.
doses, by long exposures, close proximity of the tube to the skin, or the
employment of soft tubes, the rays are capable of devitalizing the tissue
elements, interfering with the process of reproduction, and causing their
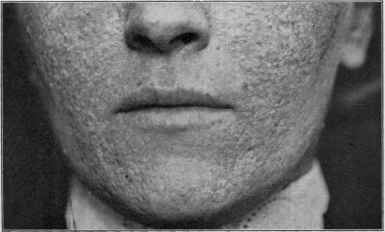
Fig. in.—Atrophic spots, somewhat depressed, coarseness of the skin, pigmenta
tion, and telangiectases, developing several months after xray exposures had been
discontinued; there was also considerable “old-age wrinkling,” but this has largely
disappeared.
degeneration; and that this power is the result of a direct specific action
of the rays; (c) that the more highly differentiated structures, such as
the hair-follicles, glands, nails, and blood-vessels, are more readily and
severely affected by the rays than the less-differentiated epidermal cells
448
INFLAMMATIONS
or the fibrous stroma of the corium; (d) that pathologically altered cells,
whether of epiblastic or mesoblastic origin, are far less resistant to the
rays than healthy cells, and are devitalized with small doses of the rays,
and that this destructive action on diseased elements may be taking
place while the healthy elements in the neighborhood, instead of having
their vitality inhibited, may be stimulated to a process of repair; (e) that
the action of the rays is cumulative, and that when the cellular degenera
tion reaches a certain degree the toxic products of the breaking-down
cells are capable of setting up an inflammatory reaction, which is a
secondary phenomenon; (f) that this inflammatory reaction is peculiar
in that it occurs in a tissue the vitality of whose various elements has
already been impaired by the action of the rays, and in that it is associated
with greater destructive changes than those produced by the actinic
rays, and is apt to lead to ulceration and necrosis, and is liable to be
followed by an imperfect process of repair. Wolbach1 ascribes this
failure of repair very largely to the degenerative changes set up in the
blood-vessels.
Treatment.—The best treatment of x-ray burns is, so to speak,
their prevention. The dangers of too long and too frequent exposure,
too close proximity, and a high-current intensity are, so far as possible,
to be avoided. Leonard, Oudin, Barthélemy and Darier, and others
have advised the interposition of grounded thin or perforated sheets of
conducting material, which permits penetration of the rays, but such
a plan has not been generally followed. In the “raying” or treatment
of limited areas it is, however, advisable to protect the surrounding parts
by a thin sheet of lead. The mild and moderate forms of x-ray derma
titis require the ordinary palliative applications employed in the acute
types of eczema (q. v.) and in dermatitis from other causes. Soothing
applications are usually sufficient to bring the irritation to a more rapid
disappearance. The x-ray ulcers in most instances are obstinate, and
the most satisfactory plan in refractory cases is to curet and, if necessary,
skin-graft. In such patients, where operation, for the time at least, is
not feasible, the local applications are to be the mildest possible; oint
ments containing cocain, opiates, menthol, acetanilid, for the control of
the intense pain, are to be variously tried. In a case under my own care
at the Howard Hospital almost all applications intensified the painful-
ness, and the only ointment giving relief was one containing 1 or 2 drams
(4.-8.) of orthoform to the ounce (32.). No progress was made in this
case toward healing, and a year or so later the area was curetted and skin
grafted by my colleague, Dr. C. H. Frazier, and recovery finally resulted.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |