| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
SCLERODERMA1
Synonyms.—Hidebound skin; Sclerema; Scleriasis; Sclerema adultorum; Derma-
tosclerosis; Fr., Sclérodermie; Sclérème des adultes; Ger., Sklerodermie.
Definition.—A chronic disease, characterized by a circumscribed
localized, or general and more or less diffuse, usually pigmented, rigid,
stiffened, indurated, or hidebound condition of the skin.
The manifestation differs materially in extent and character, in
some cases being more or less diffused, hard, hidebound, and with usually
considerable pigmentation, and in others consisting of rather sharply
circumscribed patches or bands of a somewhat lardaceous appearance,
and often, especially the rounded areas, with a pinkish border. The
former is the variety usually known as diffuse symmetric scleroderma;
the latter, as circumscribed scleroderma or morphea. Duhring main
tains that morphea is distinct from scleroderma, and it must be confessed
that the extremes of these two types bear practically no clinical resem
blance, one to the other, but other cases approach more closely and merge
into each other, some cases presenting the typical conditions of both.
1 Some valuable recent literature: Lewin and Heller, Die Sklerodermie, Berlin, 1895
(a review of the entire subject, embracing 508 collected cases); Osier, Jour. Cutan. Dis.,
1898. pp. 49 and 127 (a report of 8 cases of diffuse scleroderma, with review comments
on the disease, especially diagnosis and treatment with thyroid extract); Dercum, Jour,
of Nervous and Mental Dis., July, 1896 (3 cases) and (on scleroderma and rheumatoid
arthritis—with reports of 2 cases), ibid., October, 1898; Méneau, Jour. mal. cutan., 1898,
p. 145; Colcott Fox, Brit. Jour. Derm., 1892, p. 101, also contributes an interesting
historic paper bearing upon early observations of English observers on the disease.
SCLERODERMA
579
Symptoms.—The diffuse type may begin insidiously or rapidly.
In the former event the first symptom noted is a slight stiffness of the
part involved, which may at first be extremely limited. On examina
tion, variable swelling or infiltration is usually noted, the surface is some
what tense looking, and sometimes shining; at other times there is noted,
along with the first symptoms, more or less yellowish-brown or brownish
pigmentation, and which may, indeed, be the first manifestation ob
served by the patient. As a rule, there are no subjective symptoms
complained of in the early stages, except in some cases occasional neural
gic or rheumatic pains. The division between the affected and the
healthy skin is not well defined, one insensibly disappearing into the other.

Fig. 140.—Scleroderma—band or ribbon type, extending full length of the arm.
Several “morphea” patches on back.
The process gradually extends, and, after the course of weeks or some
months or several years, finally involves one or more regions or the
greater part of the entire surface. It may be limited to the arms or the
lower extremities, extending sometimes on to the trunk; or the face,
neck, and immediately adjacent parts are the seat of the induration.
When well established the integument is brawny or leathery, hard to the
touch, stiff, rigid, and cannot be lifted up into folds. It is usually appar
ently agglutinated with the subjacent tissues, and the entire part is more
or less immobile.
In the rapidly spreading or acute type, the process is commonly
ushered in by more or less edematous infiltration, with or without
580 HYPERTROPHIES
preceding chills, fever, or other constitutional disturbance. The tissues
and skin are tense and generally glossy, and in some instances may pit
slightly upon pressure, although, as a rule, owing to the tenseness and
beginning hardening, this is not readily produced. In these edematous
or infiltrating cases the skin is often whitish or waxy, somewhat similar
to the appearances observed in ordinary edema. The disease rapidly
extends, and soon a greater part of the entire surface is invaded. The
infiltration or edema disappears as the integument becomes hard and
rigid, and practically the same picture is presented as in the insidious
form: the skin is dry, sometimes harsh, sometimes smooth, hide
bound, stiff, and hard and more or less pigmented, and not infre
quently with some shriveled epidermic scaliness. In some instances,
in places, especially the lower leg, there is slight wart-like papillary
hypertrophy.
If the limbs are involved, they are stiff and immobile, and later
become shrunken and withered, the underlying muscles also atrophying,
and the whole region—skin, tissue, muscle, and bone—seems glued
together and atrophic. In some cases (Thibiérge)1 the muscles are
noted to be atrophic, even where there is no overlying sclerodermic
areas. If the face is the part involved, the countenance is immobile,
expressionless, the wrinkles and lines obliterated, and the mouth slightly
or firmly rigid. In fact, the integument has a wooden or petrified look.
Atrophic changes may take place here also, but not so commonly as with
the extremities. When seriously involving the latter, joint symptoms
of an arthritic or rheumatoid arthritic character are noted, and, in addi
tion to the enormous shrinking and atrophy which sometimes ensue, even
to the extent of reducing the arm of an adult to almost that of a child,
the joints become ankylosed, the fingers bent and fixed, resulting in a
veritable sclerodactylia, an associated condition to which Ball called
attention, and well shown in cases more recently reported by Osier,2
Dercum.3 Elliot,4 Uhlenhuth,5 and others.6 Both the fingers and toes
may be the seat of these changes, as in some of the cases just referred to
and in one referred to by Kalischer.7 Sometimes such distortion is
preceded by pain, occasionally cyanosis, and, in fact, many of the other
symptoms of Raynaud‘s disease (Bouttier, Chauffard, and others).8
Ulcerations are apt to form over the knuckle prominences, and the whole
condition be a painful and troublesome one. In such cases and in
others often the first troublesome symptom noted is slight ulceration
1 Thibiérge, “Contribution a l‘étude des lésions musculaire dans la sclérodermie,”
Revue de Méd., 1890, p. 291, calls special attention to the characters of the muscular
atrophy observed and refers to other literature cases; Bloch, Berlin, klin. Wochenschr.,
1899, P- 307, has added a case of bone and muscle atrophy to those already reported;
also case reported by Adler, ibid.; and one by Nixon, Bristol Medico-Chirurg. Jour.,
Dec, 1903, and refers to case by Dreschfeld (Manchester Med. Chronicle, 1897, p. 263).
2 Osier, loc. cit. 3 Dercum, loc. cit.
4 Elliot, Jour. Cutan. Dis., 1899, P- 575-
5 Uhlenhuth, Berlin klin. Wochenschr., 1899, p. 207.
6 Gordonier, Amer. Jour. Med. Sci., 1889, vol. xcvii, p. 15, reports a case and re
views others.
7 Kalischer, Wien. med. Rundschau, 1899, p. 65.
8 Bouttier, “De la Sclérodermie,” These de Paris, 1886; Chauffard, abs.-ref.,
Annales, 1897, p. 895; also noted by Osier, Dercum, and others.
SCLERODERMA
58l
of the finger-ends; Jacoby‘s1 case began in the form of open sores,
the different finger-tips being successively attacked, and Eichhoff2
observed an instance somewhat similar, but in which the apparent
exciting factor of the atrophic and destructive process was a favus
of the nails. In some cases, especially those in which the subcutaneous
tissues and muscles have atrophied, the hardened skin may tend to ulcer
ate over sharp bony prominences.
The disease may, however, begin on any region, and the most fre
quent one is that of the neck, although shoulders, back, chest, arms, and
face are not uncommon sites. It may limit itself somewhat, or it may
gradually or quickly involve almost the entire surface. As a rule, it is
extensive. It may be somewhat irregular in its distribution, but it is
usually symmetric—in a case described by Britton,3 the disease was not
only diffused over most of the surface, but its symmetric character was
perfect; and in one recently noted by Bruns,4 the disease involved both
lower extremities, extending upward and stopping short level with the
second sacral vertebra. Not only may the skin be involved more or less
extensively, but the mucous membrane of the mouth as well, and this
has also been observed even when the integumentary involvement was
limited. Sometimes, too, the teeth loosen and fall out (Dercum). In
some cases the scleroderma presents in wide strips or bands, and occa
sionally associated with circumscribed areas of more or less typical
morphea, and in exceptional instances, in addition to the sclerodermic
changes, there are noted associated alopecia and leukoderma.5
As a rule, there are no distinctive or special constitutional symptoms
in scleroderma; some of the less extensive cases and most of those of
wide distribution are ushered in by chills, fever, and other evidences
of general disturbance. There are not infrequently, however, concomit
ant or developing rheumatic symptoms and occasionally those of rheu
matoid arthritis. Pigmentation is sometimes marked, and sometimes
suggestive of Addison‘s disease; in exceptional instances this latter has
been reported to coexist. Local pain, occasionally cramp-like in char
acter, heat or burning, and a sense of numbness, and, as already referred
to, edema are sometimes precursory and early accompanying symptoms.
The sweat secretion of the involved region is diminished, and usually
entirely suppressed. Sensibility of the parts is rarely affected, but there
is itching in some cases. Changes in the thyroid gland have also been
observed in some instances (Singer, Jeanselme, Ditscheim, Grünfeld,
Osier, Uhlenhuth, James, Samouilson, and others), but usually in asso
ciation with coexistent Graves’ disease. In extreme types, especially
when the face is involved, from stiffening and often contraction of
the mouth, proper nourishment is interfered with, and the patient
suffers from inanition. From hardening and contraction of the
1 Jacoby, Philada. Med. Jour., April 15, 1899.
2 Eichhofl, Archiv, 1890, vol. xxii, p. 857 (with cut).
3 Britton, Brit. Jour. Derm., 1891, p. 227.
4 Bruns, Deutsche med. Wochenschr., 1899, p. 487.
5 Eddowes, Brit. Jour. Derm., 1899, p. 325, exhibited before Derm. Soc‘y of Great
Britain and Ireland a case presenting general alopecia, leukoderma, scleroderma, and
morphea patches.
582 HYPERTROPHIES
integument of the chest breathing is also seriously interfered with in
some cases.
The course of the disease is essentially chronic, sometimes exten
sion being slow, at other times rapid. In some cases there is occa
sional retrogression, which may even go on to complete recovery, but
before such a fortunate conclusion there may occur one or more exacer
bations, usually foreshadowed by chilliness or chills and other systemic
disturbance.1 The edematous cases are more likely to lead to atrophic
changes—Crocker believes this to be the result in all of them.
Circumscribed Scleroderma—Morphea (known formerly as Keloid
of Addison).—The disease may present some variations. The typical
examples, those which seem wholly different from scleroderma, begin,
as a rule, by the appearance of light-pinkish or hyperemic, usually oval
or rounded, small coin-sized patches. There may be slight elevation
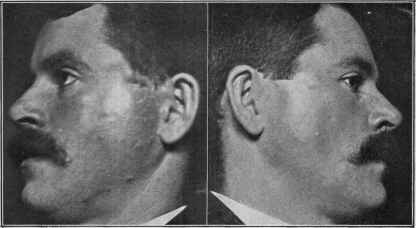
Fig. 141.—Circumscribed scleroderma (morphea) in a man aged thirty; consisting
of two symmetric areas shown, which were waxy or lardaceous in appearance, quite
firm to the touch, and with a slight peripheral, pinkish border, although this was not at
all marked and discernible only upon close inspection. Duration one year and of
gradual appearance.
or an appearance of scarcely perceptible puffiness. The color, in the
course of some days—a variable time—fades out, and the patch is ob
served to be encircled with a faint rosy or pinkish zone, which, on close
examination, is found to be made up of minute capillaries, while the area
itself is whitish or ivory-like, or lardaceous, and seems inlaid in the skin.
It is usually on a level with the surface, or it may be slightly depressed;
it often has a polished look, and it is either somewhat soft to the touch,
and when pinched up not materially different from the surrounding
skin, or it is noted to be firm, hard, leathery, and even brawny. On
close inspection very often the surface is observed to be coursed over by
1 An interesting paper and review in this connection: Kanoky and Sutton, “A Com
parative Study of Acrodermatitis Chronica Atrophicans and Diffuse Scleroderma, with
Associated Morphea Atrophica,” Jour. Cutan. Dis., Dec, 1909 (illustrated, bibliog
raphy).
SCLERODERMA
583
minute blood-vessels, sometimes forming a faint network. Later,
instead of a smooth, shining surface, there may be slight, thin, shriveled
epidermic coating. Beyond the faint pinkish, or sometimes lilac-
colored, border, a slight yellowish or yellowish-brown, often mottled,
irregularly diffused pigmentation is noticeable, which may extend some
distance from the patch.

Fig. 142.—Circumscribed scleroderma (morphea) in a middle-aged working-
woman; disease limited to the patch shown on the leg. Duration about one year. The
pinkish or lilac border present in most cases is shown by the dark peripheral shading.
The inclosed area is whitened and lardaceous in appearance. The two small ulcera-
tions are accidental, due to traumatism.
In some instances the patches, instead of being pinkish or rosy,
begin as whitish or bluish-white (Handford1) areas, later becoming yel
lowish. In exceptional instances the erythematous stage usually
noticed is prolonged. As a rare example of this latter was one under
Cavafy‘s2 observation, in which the legs were for months the seat of
1 Handford, Illus. Med. News, June 22, 1889, p. 265, records, in a report of 2 cases,
a case of this kind (with colored plate and histologic cut).
2 Cavafy, Brit. Jour. Derm., 1896, p. 275.
584
HYPER TROPHIES
erythematous areas of obscure nature, but which finally began to
harden, the erythema disappearing and giving place to lardaceous
patches. In other instances, instead of the typical characteristic patches,
there appear several or more small or large scar-like spots, sometimes
slightly depressed; the skin is atrophic or thin, and often with neighbor
ing telangiectases of reddish or bluish color. Pigmented areas, true
sclerodermic areas, pit-like atrophic depressions, and atrophic lines are
also present in some cases.1 Or, instead of lesions of these characters,
the disease may present in irregularly rounded areas, or short or long
bands, hard and brownish, sometimes with the peculiar pinkish capillary
border or with abrupt termination in the skin beyond, which may or
may not be pigmented. Occasionally a band extends almost the entire
length of a limb, and may be elevated or countersunk. In these cases
paroxysmal attacks of cramp-like pain are now and then noted.
The course of the typical lesions of morphea is variable—usually
slow and chronic in character; they frequently enlarge slowly, and if
close together, coalescence results, and large areas may be covered.
Very often after reaching the diameter of a few inches they remain
stationary for an indefinite time, either with a gradual tendency to
enlargement or to retrogression and disappearance. In some cases
decided atrophic changes ensue, and the final result is akin to that ob
served in diffuse scleroderma: the skin is shriveled and thin, and some
times hard and fibrous, the tissues beneath gradually atrophy, and the
parts agglutinated together, finally forming irregular, smooth or fur
rowed, sunken, contracted scars, sometimes of keloidal aspect or nature.
In rare instances ulceration takes place, usually in parts of the involved
area only.
Morphea patches may develop upon any region, but its most com
mon sites are the upper trunk, face, neck, abdomen, and the arms and
thighs; as a rule, but several areas are seen, but it may be widespread
over several regions, as in extensive cases described by Morrow2 and
Cavafy,3 in which there were numerous large areas from the hips down
on both legs, and with more or less perfect symmetry. Ordinarily patches
of the disease are irregularly distributed, sometimes presenting on but
a single region; occasionally the distribution corresponds to that of the
cutaneous nerves, and exceptionally the manifestation has been strictly
limited to the fifth nerve, as in Anderson‘s4 case, in which the entire
region of the distribution of the three divisions of the right fifth nerve
was the seat of sclerodermic changes, including the mucous membrane
of the mouth and the upper part of the pharynx. Barrs5 observed a
case in which the disease, upon both arms and left leg, followed very
accurately the nerve-fields.
In rare instances, closely analogous to the last, as in a case also
1 Duhring, Amer. Jour. Med. Sci., Nov., 1892, reports an interesting case of asso
ciated morphea patches and atrophic lines and spots.
2 Morrow, Jour. Cutan. Dis., 1896, p. 419 (with 3 illustrations) and discussion
(White and Duhring), p. 446.
3 Cavafy, loc. cit.
4 W, Anderson, Brit. Jour. Derm., 1898, p. 46.
5Barrs, ibid., 1891, p. 152.
SCLERODERMA
585
reported by this last observer (Barrs), as well as by others previously,
the disease seems to limit itself, chiefly at least, to one side of the face
(hemiatrophia facialis or unilateral atrophy of the face), but not infre
quently with one or several characteristic patches elsewhere. With
these cases, however, the atrophic “shrinking” influence of the disease
is especially noticeable, not only the skin, but the subcutaneous tissue
muscles, and even the bones becoming involved, and great deformity
sometimes resulting.
Etiology.—Both types of scleroderma are infrequent—the dif
fused type rare, the circumscribed variety—morphea—much less so.
It is met with in both sexes, but with a considerable preponderance
on the female side, and this, I believe, is even more pronounced in
morphea. In Lewin and Heller‘s statistics, out of 435 cases, 292 were
females. It is chiefly observed in those between the ages of fifteen
and forty-five, but no age except early infancy is exempt, as it has been
met with both in the very young (the youngest patient recorded being
thirteen months old) and the very old. Various causes have been as
signed, but there remains much to be learned before anything definite
can be stated on this score. Rheumatism, chills, exposure to cold and
wet, prolonged sun-exposure, thyroid disease, exhaustion from any cause,
emotional and other nervous disturbances, filaria sanguinis (Bancroft),
arterial disease, and many other factors are named as of etiologic in
fluence. Some cases have apparently had their start in some local
irritation or injury, another example of which is recently recorded by
Leslie Roberts.1 In some instances, however, the patients at the time
of the attack are apparently in good health, and when the involvement
is not unusually extensive, the general condition may remain compara
tively undisturbed; this is especially so in most cases of morphea.
Zambaco2 is inclined to view the disease as an anomalous or modified
form of leprosy.
The rheumatic origin of the disease has the frequent occurrence
of rheumatic and rheumatoid arthritic symptoms to support it, such
symptoms sometimes antedating the sclerodermic changes, and in other
cases being concurrent. These facts are, however, in my judgment,
more especially as to rheumatoid arthritis, merely an added evidence
in favor of the neurotic cause of the disease, which, upon the whole,
has the greatest support. That changes in the thyroid gland are noted
in some cases has already been remarked upon, usually, however, in
association with Graves’ disease, but also in some instances in which
this latter did not exist, usually atrophic in character, as reported by
several observers, more recently by Hektoen,3 Uhlenhuth,4 James,5 and
others.6
1 Roberts, Brit. Jour. Derm., 1900, p. 118.
2 Zambaco, Trans. First Internat. Leprosy Congress.
3 Hektoen, Jour. Amer. Med. Assoc, June 26, 1897, vol. xxviii, p. 1240.
4 Uhlenhuth, Berlin klin. Wochenschr., 1899, p. 207.
5 James, Scottish Med. and Surg. Jour., May, 1899.
6 Samouilson, “De la Coéxistence de la sclérodermie et des altérations des corps
thyroide,” These de Paris, July 21, 1898, considers the subject at length and reviews
the literature, with the conclusion that the disease is sometimes due to an intoxication
resulting from abnormal action of the thyroid gland; Leven, Dermatolog, Centralblatt,
586 HYPERTROPHIES
In favor of its being a neurosis are the occasional nerve distribu
tion, its frequent symmetric arrangement, the occasional preceding or
concurrent finger symptoms, suggesting Raynaud‘s disease, the occasional
local sensory symptoms, the sometimes noted coexistence of alopecia
and leukoderma, the pigmentary changes, the muscle and bone atrophy,
etc.
Pathology.—Knowing so little regarding the essential causes
which provoke the disease, it is difficult to formulate a satisfactory
explanation of the pathologic changes which take place in the cutaneous
structures. As Osier succinctly states, as already in part intimated in
etiology, the disease is variously regarded as a trophoneurosis dependent
upon changes in the nervous system—a perversion of nutrition analogous
to myxedema, and due to disturbance of the thyroid function; a sclerosis
following widespread endarteritis; a primary slow hyperplasia of the
collagenous intercellular substance of the corium—fibromatosis; or a
primary affection of the lymph-channels, central or peripheral. Lewin
and Heller, from their valuable studies, are led to view the disease as a
neurosis—an angioneurosis, trophoneurosis, or angiotrophoneurosis. As
Crocker states, most of the symptoms can be referred to obstruction,—
arterial, lymph, and venous,—and that the variable character of changes
observed in different cases depends upon which of the vascular sys
tems is most involved. According to Unna, the first changes are in
the connective tissue, especially its intercellular substance. It is
probable that the primary pathogenic influence is to be found in the
central nervous system, although many (Chiari, Spieler, Dinkier, and
others) have failed to find such evidence; but, on the other hand, West-
phal,1 Jacquet and de Saint-Germain,2 Schulz,3 and Steven4 have noted
degenerative and sclerotic changes in the brain, spinal cord, or sympa
thetic, but there was no uniformity, and the exact relationship cannot,
therefore, be definitely stated. Brissaud5 believes it takes its origin in
some disturbance of the sympathetic. In Schulz‘s case, in which there
was considerable general pigmentation, one suprarenal body was found
somewhat diseased.
The anatomic changes observed in the diffuse type (Neumann,
Kaposi, Auspitz, Schwimmer, Fagge, and others) are essentially in the
corium and subcutaneous tissues. Pigmentation, it is true, is found in
the rete, and not infrequently in the corium also, especially in the papil-
Feb., 1904 (associated development of thyroid); Roques, “Le Traitement opothéra-
pique de la sclerodermie,” Annales, July 1910, p. 383, reviewing the subject, found
a larger proportion with defective thyroids; full review of literature; bibliography;
Alderson, “The Skin as Influenced by the Thyroid Gland,” California State Jour, of
Med., June, 1911, (gives a brief, but good review of recorded thyroid gland influences).
1 Westphal (2 cases—1 autopsy), Charité-Annalen, Berlin, 1876, vol. iii, p. 341.
2 Jacquet and de Saint-Germain, Annales, 1892, p. 508.
3 Schulz, “Sclerodermie, Morbus Addisonii und Muskelatrophie,,, Neurologisches
Centralblatt, 1889, pp. 345, 386, and 412, with references.
4 Steven, Glasgow Med. Jour., Dec 1898; editorial review of same in Lancet, 1899,
vol. i, p. 43; clinical account of case in Internat. Clinics, July, 1897, vol. ii, p. 195,
with 4 illustrations (an interesting case leading to pronounced hemiatrophy of the face,
body, and extremities, with deformity and fibrous ankylosis of the joints).
5 Brissaud, La Presse médicate, 1897, p. 285—full abstract in Brit. Jour. Derm.,
1897, p. 367—reviews the various theories (with many references).
SCLERODERMA
587
lary layer. Both in the true skin and subcutaneous connective tissue
there is a marked increase of connective-tissue element, with thickening
and condensation. The fat atrophies and gives place to connective
tissue. The vessels are found surrounded by masses of small cells of
unknown origin, and are thereby diminished in caliber; the latter is also
due to thickening of the media and intima. The glandular structures
are irregularly surrounded by these cell-masses, but are primarily other
wise unchanged; in the later stages, however, they are atrophied. Ex
cepting the presence of these cells there are no inflammatory signs.
The papillae are usually normal in size, although in some cases in which a
papillomatous tendency is noted hypertrophy is observed. The con
nective tissue and elastic tissue of the corium are increased, densely
packed, and the entire cutaneous structure is converted into a dense
mass. The histologic changes in the circumscribed form, studied
carefully by Crocker, vary relatively little from those of the diffused
type in its early stage, both having the same anatomic basis, the cell
exudation bringing about the first change—narrowing of the vessels,
fibrillar tissue formation, and atrophic changes; the pinkish or violaceous
zone is due to collateral hyperemia around an anemic area. Duhring
found in a soft, pliable, whitish patch of some months’ duration a con
densation of the connective tissue of the corium, with a shrinkage of the
papillary layer.
Diagnosis.—In well-marked cases of diffused scleroderma the
characters—rigidity, stiffness, hardness, and hidebound condition of
the skin, with usually more or less pigmentation—are quite distinctive
and scarcely admit of error. In the less marked and obscure examples
possible confusion might occur with Raynaud‘s disease, the brawny
induration sometimes observed in scorbutus, myxedema, and leprosy,
but the features and mode of onset of these several affections are clearly
different. The nervous phenomena, the usually preceding and long-
continued and often periodic stasic and anemic conditions of the favorite
limited regions in Raynaud‘s disease, are differential points of value,
and together with the absence of any tendency to extensive hardening
or thickening will usually serve to prevent a mistake in this direction.
The localization of the brawny hardness of scurvy, the purpuric element,
and other symptoms are distinct from those of scleroderma. The
edematous stage observed in some cases presents a similarity to myx-
edema, but the distribution and mode of onset of the latter, the absence
of sclerotic and other features, are different. Leprosy can scarcely be
confounded with diffuse scleroderma, the sensory disturbances usually
present and often preceding the development of the cutaneous symptoms
in the former, the absence of tendency to brawny hardening, the history
of the case, and the exposure to the disease are points to be considered.
The malady can scarcely be mistaken for xeroderma pigmentosum.
Sclerema neonatorum, a somewhat allied disease, is an affection of
earliest infancy, whereas scleroderma has never been noted before the
second year of life.
The early white plaques of morphea—circumscribed scleroderma—
in some cases resemble closely similar areas not infrequently seen in
588
HYPERTROPHIES
leprosy, but the symptoms and characters of the latter already noted are
of different nature. The morpheic white areas may also bear resem
blance to vitiligo, but in the latter the sole essential symptom is loss of
pigment—no thickening or other change in the skin. In women a mis
take between carcinomatous skin invasion of the breast (cancer en
cuirasse) and the circumscribed sclerodermic disease has been made, but
careful investigation should prevent error.
Prognosis.—The outcome in a given case of either variety as
regards cure is uncertain; the diffused type is often fatal, usually from
some intercurrent affection superinduced by the patient‘s condition.
In those in which the chest is practically incased in an unyielding armor,
and the mouth narrowed and fixed, and the jaws firm, interfering with
respiration and nutrition, the prospect is unfavorable. According to
Méneau, the scleroderma, progressive in character, beginning at the
extremities and spreading to other parts, is generally fatal. On the other
hand, in many extensive cases and seemingly unfavorable, if decided
atrophic changes have not occurred, recovery takes place.
The circumscribed form—morphea—is a relatively mild affection,
often persisting, it is true, and in some cases, almost indefinitely, but is
not necessarily dangerous, and very often, after some months or a year
or two, either as the result of treatment and sometimes spontaneously,
complete recovery ensues. Considerable deformity may, however,
result in the rarer instances in which atrophy takes place.
Treatment.—The patient‘s general health must receive proper
attention, and such tonics as quinin, strychnin, iron, arsenic, sodium
salicylate, and cod-liver oil have an important influence in some cases.
Of these, several—arsenic, sodium salicylate, and cod-liver oil—have in
my experience been the most valuable, and probably possess more than
a simple tonic and alterative value. My own observations, however,
have concerned, for the most part, the circumscribed forms of the disease.
In extensive cases, in addition to those remedies named, the adminis
tration of pilocarpin, properly supported with stimulants and tonics,
and its action on the sweat-glands promoted by warm clothing or bed-
covering, is of some value when the sweat secretion is markedly in
abeyance. Recently thyroid extract has been advocated, but the re
ports are at variance. Osier has not been favorably impressed with its
use, although still recommending its trial. The cases mentioned by
Lewin and Heller, in which this treatment was adopted, were not ma
terially influenced, and this was also the experience of Uhlenhuth,
Dreschfeld,1 and some others. On the other hand, Marsh,2 Lustgarten,3
Gayet,4 Eddowes,5 Roques,6 and others have seen betterment take place.
As yet, therefore, the exact value of this remedy remains to be deter
mined—it should, however, be tried, in all diffused cases at least.
The local treatment most efficacious consists essentially in the use
1 Dreschfeld, Medical Chronicle, 1896-97, vol. vi, p. 263.
2 Marsh, Med. News, 1895, vol. lxvi, p. 427.
3 Lustgarten, Jour. Cutan. Dis., 1895, p. 27 (brief reference only).
4 Gayet, Jour. mal. cutan., Jan., 1900.
5 Eddowes, Brit. Jour. Derm., 1899, p. 325.
6 Roques, loc. cit.
SCLEREMA NEONATORITM
589
of friction with oils or ointments and massage. The applications should
usually be of mild character, or in limited, obstinate, non-irritable areas,
quite stimulating. As a mild ointment may be mentioned one contain
ing salicylic acid 10 grains (0.65), cacao-butter 2 drams (8.), lanolin
2 drams (8.), petrolatum 4 drams (16.); or 1 or 2 per cent, salicylated
oil can be used. In the hard, thickened, sclerodermic areas in the cir
cumscribed form I have used with advantage an oil consisting of 1 or
2 parts of oil of turpentine with 6 parts oil of sweet almonds; and an oint
ment of 2 parts oil of turpentine, 1 part beta-naphthol, 2 parts oil of
sweet almonds, and 10 parts lanolin; and in the tough band areas on the
extremities, sometimes associated with paroxysmal pain, an ointment
containing 5 or 10 grains (0.35-0.65) of menthol and \ dram (2.) of chloro
form to the ounce.
In the typical soft or moderately hard areas of morphea, especially
in the earliest stages, the mild applications are to be used, the stronger
sometimes tending to produce irritation. Electric treatment, consist
ing of general and local galvanization, has been commended by some
observers; with the former I have had no experience, but the latter,
using a current of 2 to 10 milliampères, with friction movements of the
two electrodes—labile application—has seemed to me of some advantage;
likewise the use of the static battery roller electrodes made over the part,
while covered with the clothing or some fabric. In the past few years
favorable statements have been made of electrolysis in the treatment of
circumscribed patches by Brocq,1 Darier and Gaston,2 and Allen.3
I have had no experience with this method. It is employed in the same
manner as in the removal of superfluous hairs: current strength between
½ to 10 milliampères, according to sensitiveness of the patient and the
integumentary conditions; the stronger current in the more infiltrated
areas, if the patient bears it, and in such cases, too, the duration of the
application somewhat longer than in the softer and less infiltrated patches.
Brocq employs as supplementary to the electrolytic procedure the ap
plication of mercurial plaster, which, I believe, should have a share in
the credit for the good results claimed by him. X-ray treatment is some
times especially valuable in the morphea type of the disease.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |