| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
CLASS IX—PARASITIC AFFECTIONS
A. DISEASES DUE TO VEGETABLE PARASITES
FAVUS
Synonyms.—Tinea favosa; Tinea ficosa; Tinea lupinosa; Tinea maligna; Tinea
vera; Porrigo favosa; Porrigo lavalis; Porrigo lupinosa; Porrigo scutulata; Derma-
tomycosis favosa; Porrigophyta; Trichomykosis favosa; Crusted ringworm; Honey
comb ringworm; Fr., Teigne faveuse; Teigne du pauvre; Teigne rural; Ger., Erbgrind.
Definition.—Favus is a contagious, vegetable-parasitic disease
of the skin, characterized by pin-head to pea-sized, friable, cup-shaped

Fig. 270.—Favus, in a woman aged twenty-three, of some years’ duration; showing hair
loss, atrophic thinning of the skin, and the cup-shaped crusts at peripheral portion.
yellow crusts, tending sooner or later to form coalescent, mortar-like
masses.
Symptoms.—The common and usual site of favus is the scalp,
but it may occur upon any portion of the integument, and occasion
ally attacks the nails (see Onychomycosis). To the latter regions it
is usually conveyed from the disease on the scalp, although it does occur
1093
1094
PARASITIC AFFECTIONS
sometimes primarily upon the non-hairy surface, and to which it may
indeed be limited. The nails are rarely the primary seat of the malady.
In favus of the scalp, sometimes designated tinea favosa capitis,
favus pilaris, the affection develops, as a rule, insidiously and slowly,
beginning as an insignificant superficial inflammation or merely as a
hyperemic spot; in the earliest stage or period this is more or less cir
cumscribed and slightly scaly, the scaliness being usually of a thin,
branny character. There is soon noticed the appearance of yellowish
points at the hair-follicle outlets, surrounding the hair-shaft. These
yellowish points or crusts increase in size, growing slowly, becoming ordi
narily the area of small peas; they are cup-shaped, with the convex
side pressing down upon the papillary layer of the skin, and the concave
side facing externally, constituting the so-called favus scutulum. They
are raised several lines above the surface level, are friable, sulphur-
colored, and usually, in the beginning at least, each cup or disc is pierced
by a hair. Some show distinct concentrically disposed furrows. Upon
removing the crust the underlying surface is found to be somewhat
excavated, reddened, and if the malady has existed for some time, also
atrophied; exceptionally it is suppurating. In detaching the disks, more
especially those of some duration, slight serous exudation or even bleeding
is sometimes noticed. As the disease continues and progresses, the
crusted points or spots extend somewhat, new ones arise in the inter
spaces, and, as a result, the crusts become more or less confluent over
the involved area, and form irregular masses of thick, yellow or yellowish,
mortar-like accumulations. While the crusts are yellowish, and at first
a clear yellow, later, from the admixture of extraneous matter, they often
have a brownish tinge. They have, when present in any quantity, a
peculiar, characteristic odor, which has been likened to that of stale,
musty straw, to that of mice, and the urine of cats.
The progress of the malady is exceedingly slow, so that months
often elapse before there is much involvement, the disease sometimes
limiting itself to an irregular area of one or two inches in diameter.
Not infrequently, while the first patch increases gradually, new foci
show themselves in one or more near-by or remote parts of the scalp.
In some instances, especially near the border of the crusts, are seen
pustules or suppurating points, and exceptionally the whole involved
area may exhibit slight or moderate suppurative action, by which the
accumulated masses are in places loosened and cast off; this latter
usually occurring after the malady has been of some duration, during
which time the hair of the affected surface, or most of the hairs, have
loosened and fallen out.
The hairs, in fact, are involved early in the disease; they become
brittle, lusterless, break off, some splitting up, and many falling out.
After a time the crusts may disappear here and there over the oldest
part, leaving an atrophic, thinned-looking, more or less hairless sur
face, with scanty or numerous, scattered, yellowish point, cup-shaped
disks or small confluent crusted spots; at the border of the area the dis
ease is still noted to be active, and presenting the ordinary symptoms
already described. The disease may thus gradually invade more or
FAVUS 1095
less of the entire scalp, and may remain active over the entire involved
surface, which is covered with the yellowish, mortar-like masses. In
sluggish, long-continued cases, in which, in most parts, the malady has
ceased to exist or to be active, there is a more or less general scurfiness,
with irregularly dispersed, small, flattened, yellowish, scaly spots; the
skin is atrophic, dry, harsh, and relatively or completely hairless, usually,
however, with small or large dry tufts here and there.
Favus of the general surface or non-hairy parts, or tinea favosa
epidermidis, exhibits symptoms essentially similar to those upon the
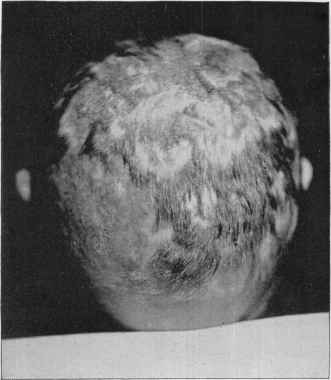
Fig. 271.—Favus, in a Russian boy aged fourteen, of eight years’ duration, showing
the extensive atrophic, cicatricial, hairless areas left. Disease only active now pos
teriorly, and to a slight extent to the right anteriorly, from which the crusts have been
removed.
scalp, beginning at the lanugo hair-follicles. In some instances, how
ever, there is tendency to the circinate patch (favus circinatus), with
the outer part more or less inflammatory, sometimes papulovesicular
(favus herpeticus), and studded with small yellow points and favus
scutula; the central portion tending to clear up, presenting a resemblance,
barring the yellowish points and disks, to ringworm. There may be one
or more of such areas. Exceptionally a patch consists of several concen
tric rings. In most cases, however, the disposition to massing similar
to that observed on the scalp is exhibited, although the masses are more
1096 PARASITIC AFFECTIONS
apt to have a rough and irregular surface. In most instances, especially
if neglected, the malady spreads rather rapidly, and often involves large
areas and is somewhat widely
distributed.1 The rapidity of
its extension is apparently in
creased by conditions of ill
health.2 While usually per
sistent, especially when more or
less extensive, it is very much
less so than the disease on the
scalp; and in extremely limited
body cases often tends to spon
taneous cure. In some in
stances marked atrophy of the
underlying skin results, and
occasionally distinct ulcera-
tion.3
While favus is a disease of
the cutaneous surface, it is pos
sible in rare instances that the
mucous membranes may be
come implicated.4 It has in a
few cases been observed on the
glans penis.5
The subjective symptoms in
favus are rarely pronounced and
sometimes entirely absent; itch
ing, varying in degree, is occa-
1 See paper by Cantrell and Stout,
“A case of Favus of the Head and
Body,” Jour. Cutan. Dis., 1894, pp.
375 and 419 (with review of similar
cases and bibliography).
2 Malcolm Morris, Brit. Jour.
Derm., 1891, p. 101 (with illustration),
and Montseret, La presse méd., No. 40,
1898, p. 254, both report a case involv
ing the general surface in phthisical
subjects, in whom, during the last stage
of the constitutional malady, there was
rapid spread of the favus.
3 In an instance observed by Hallopeau, and one by Vidal, referred to in Wick-
ham’s Paris letter to Brit. Jour. Derm., 1890, p. 149, the ulcerative action was quite
marked.
4 Kaposi, Wien. med. Presse, 1884, p. 1375, reports a case of generalized favus in
which, the patient dying subsequently from gastrointestinal disease, Kundrat (“gastro
enteritis favosa,” Wien. med. Blätter, 1884, p. 1538), found at the necropsy the favus
fungus in the esophagus, stomach, and intestine, some of which in the last had under
gone putrefactive change.
5 Glück, Archiv, 1899, vol. xlvii, p. 339 (with colored plate), noted an instance in
which, in addition to several patches on the outer surface of the prepuce, there were some
typical crusts on the corona and glans.
6 This is the case reported by Cantrell and Stout, entering the Philadelphia Hospital
just at the end of Dr. Cantrell's term, coming subsequently under my care.
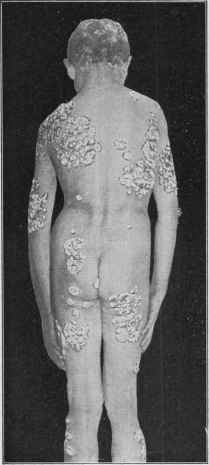
Fig. 272.—Favus—generalized—in an
Italian boy aged ten; on scalp of several
years’ duration, on general surface some
months.6
FAVUS 1097
sionally somewhat troublesome; there may also be in the suppurative
conditions some soreness.
Etiology.—Favus is due solely to the invasion of the cutaneous
structures, especially the epidermal portion, by the vegetable para
site, the achorion Schönleinii. It is seen in both sexes, but much more
frequently in males; it may occur at almost any age, but it is rare for
the scalp disease to begin after the age of fifteen. Hutchinson1 found
in 44 cases the latest age at which it began was seventeen; this patient,
when coming under notice, was aged twenty-nine, the oldest of the 44,
having had the disease twelve years. It is a contagious malady, but
relatively much less so than ringworm. It is conveyed from one person
to another, or to man from the lower animals, such as cats, dogs, rabbits,
fowl, mice, and sometimes cattle2 and the horse. It is probably communi
cated occasionally by cats, the latter contracting it from rats and mice,
especially the latter;3 but Sabouraud’s observations, as well as those of
other investigators, throw doubt upon such communication—at all
events think that such transmission is exceedingly rare. Its conta
giousness seems, however, somewhat variable, single cases often existing
in a family for years, without any other member becoming involved,
although striking exceptions are sometimes noted.4 The malady is much
more common among certain nationalities than others; it is compara
tively frequent in Northern Italy, Southern France, Russia, Poland,
Austria, Germany, Hungary, and in Scotland.5 In England and in the
1 Hutchinson, “Clinical Report on Favus,” Med. Times and Gaz., 1859, vol. xix,
p. 553 (with analytic table of 44 cases).
2 Gigard, “Sur une épidémie de teigne faveuse sivissant a Nantoin chez les bêtes
cornes et chez les enfants,” Lyon médicate, 1880, vol. xxxiv, p. 457, recorded its occur
rence at about the same time in 16 cows and 4 children in a French village.
3 See interesting paper by Sherwell, American Veterinary Review, Nov., 1892, de
tailing the contraction of the disease by 4 members of a family through the intermediary
of the dog, the latter contracting it from affected mice; Hutchins, Jour. Cutan. Dis.,
1895, p. 377, records a case in a negro, who apparently caught it from pet white rats;
Adamson, Brit. Jour. Derm., 1911, p. 49, met with 3 cases of mouse favus (achorion
Quinckeanum) in human beings, and is inclined to believe that it is not so rare as com
monly believed.
4 Crocker, Diseases of the Skin, third ed., p. 1272, noted its occurrence in 3 chil
dren of a family, one after another, the disease being primarily contracted from a cat;
Robinson (discussion), Jour. Cutan. Dis., 1895, P. 217, had under observation 3 cases
in the same family, and Allen, ibid., a case in an Irish woman, whose 3 children con
tracted the disease; Duhring, Diseases of the Skin, third ed., p. 596, refers to an
instance where 13 members of one family were in the course of years affected, and
another of mother and 2 children, constituting the whole family; in 17 cases ob
served by J. C. White (“Analysis of 5000 Cases of Skin Diseases”), Boston Med. and
Surg. Jour., 1876, vol. xciv, p. 565, more than half were instances where 2 or 3 mem
bers of the same family were affected; in 50 cases observed by Bodin, Annales, 1894,
p. 1220, more than half the patients alleged that they had caught it from others, and
10 had been in contact with affected animals; in 10 cases its origin could not be traced;
I have met with several instances of its occurrence in 2 of a family; Crary, Bull. Lying-
in Hospital, New York, May, 1904, vol. i, No. 6, reports a case in a child fourteen days
after birth, appearing on face, scalp, and elbow; the mother having the disease upon the
scalp.
5 In France its frequency is shown by Feulard, Trans. II Intemat. Derm. Cong.,
Vienna, 1892, p. 393, and Annales, 1892, p. 1118, from statistics taken from the French
Army Department; between 1876-80, of those examined for army service (at the age
of twenty), 1541 had favus; 1881-85, 1399; 1887-91, 964, the malady showing a some
what rapid decrease, but it is much more common than these figures indicate, inasmuch
as the disease is chiefly seen in children and adolescents.
In Belgium, Thomson (Clinique, Brussels, 1894, vol. viii, p. 52—abs. in Brit. Jour.
1098
PARASITIC AFFECTIONS
United States it is relatively uncommon, and with us is seen chiefly
among immigrants from the countries named;1 generalized favus is espe
cially rare in native-born Americans.2
Favus of the non-hairy or general surface, except the instances
of slight, limited patches sometimes seen, is usually consecutive to
the disease on the scalp, and in extensive types almost invariably so,
although Lustgarten3 has reported a case of the latter, the eruption
covering a large portion of both legs, in which the scalp was wholly free.
The nails (see Onychomycosis) are only rarely invaded by the favus
fungus, and then almost always secondarily, from scratching the affected
scalp.
While favus is met with over the entire world, its prevalence is
apparently greatly influenced by nationality, lack of personal cleanli
ness, neglect of the scalp,, and probably some inherent peculiarity of
the skin. It is commonly believed that a damp, moist climate favors
its occurrence, but this does not seem borne out by the facts. It is
essentially a disease of the poor, ill-fed, and uncared for, although
occasionally seen in those of fair or good circumstances and surroundings.
There is scarcely doubt but what an integument whose resisting power
has been impaired by ill health, improper and insufficient food, etc.,
becomes a readier soil for the successful inoculation and growth of the
fungus. Its much more rapid spread in the body cases during the last
stages of phthisis in the instances named points to this conclusion.
Pathology.—The achorion Schönleinii is a vegetable parasite
first discovered by Schönlein in 1839, and later by Gruby and Wedl,
although Remak was the first to confirm its pathogenic character by
successful inoculation, and who gave it the name in honor of its dis
coverer. It consists of mycelium and spores, existing in such profusion
that it is readily detected. The spores are usually rounded or ovalish,
often somewhat elongated, and vary from 0.0023 to 0.0052 mm. in
diameter (Duhring). The mycelium is composed of narrow, appar
ently flattened tubes or threads, which ramify in all directions without
definite arrangement; they average from 0.0023 to 0.003 mm. in di
ameter, and vary greatly in length, and are straight, curved, bent or
crooked, or inclined to branch in a forked manner; and sometimes they
are divided or broken up in such a way as to have the appearance of the
Derm., 1894, p. 156) shows its great frequency in that country; between 1888-92 there
were exempted from military service, owing to the disease, 3.03 per 1000, and even with
rigid examination of the recruits it exists in the service to the extent of 0.15 per 1000.
In Scotland, McCall Anderson gives (Lancet, 1871, ii, pp. 672 and 742) 156 cases
in 10,000 consecutive dispensary skin cases, or 15.6 per 1000.
In England, according to Crocker, it is observed in only 1 of 2000 consecutive skin
cases.
1 In the United States the statistics of the American Dermatological Association
show 3.43 per 1000, most of the patients, however, being foreign born. In 36 cases
under my care (20 at the Philadelphia Dispensary for Skin Diseases in a period of ten
years, and 16 in the Philadelphia Hospital in a period of five years, Philadelphia Hos
pital Reports, 1896, vol. iii, p. 176) the patients were of the following nationalities:
American born, 5; Russian, 10; Austrian and German, 10; Italian, 3; Irish, 3; Rou
manian, 2; Hungarian, 1; English, 1; and Canadian, 1.
2 Stout, New York Med. Jour., June 20, 1908, p. 1182, reports a case, scalp, nails,
arms, and legs being invaded.
3 Lustgarten, Jour. Cutan. Dis., 1895, p. 217 (with illustration).
FAVUS
1099
links of a chain (Duhring). As the disk-like scutulum and the mortar-
like mass are composed almost wholly of the fungus, there is no difficulty
in demonstrating its presence. For the examination a portion of the crust
is placed on a slide in a few drops of liquor potassæ, the cover-glass placed
over it, and allowed to stand for several minutes or longer; the cover-
glass is then pressed down, and an examination made with a power of
300 to 500 diameters. If an affected hair is examined, the same steps are
taken, except that a longer time should be allowed for the action of the
liquor potassæ, and sometimes a stronger potash solution could be used
with advantage.
According to Robinson,1 as well as to the investigations of others,
“the parasite first obtains a lodgment in the funnel-shaped depression
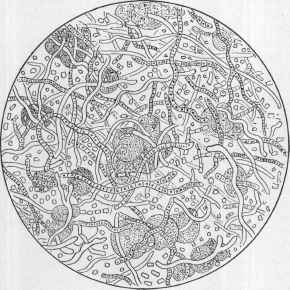
Fig. 273.—Favus fungus—achorion Schönleinii (X about 700; partly diagrammatic).
in the epidermis through which the hair-shaft emerges upon the surface.
It grows luxuriantly in the upper part of the hair-sac, and insinuates
itself on all sides between the superficial layers of the epidermis. When
it reaches a short distance on all sides of the follicle-mouth, it breaks the
looser layers and appears on the surface, giving us the familiar cup-
shaped bodies. It also invades the hair-shaft itself, though not to the
extent that the ringworm parasite does. It penetrates between the
cellular layers of the root-sheath, and multiplies in the cortical substance
of the hair. The nutrition of the hair is interfered with by the mechan
ical pressure of the growth upon the papillæ. The hair falls out, and
eventually in many cases the papilla atrophies and a new growth becomes
impossible. In cases of any standing the parasite may be demonstrated,
not only in the cortical but in the medullary substance of the hair.
1 Robinson, Manual of Dermatology, p. 605.
1100 PARASITIC AFFECTIONS
Splitting of the hair may occur, as in ringworm, but as a usual thing the
hair falls out before that occurs.” “In the skin itself the parasite usually
confines itself to the upper corneous cells, and does not extend to the liv
ing tissues.1 In cases where the surface is covered by irregular, mortar-
like masses of the parasite, the entire upper layer of the epidermis will be
found infiltrated with the achorion. The corium itself is usually in a
state of chronic inflammation, and suppuration, which may be quite
abundant, often occurs under the crusts. Even where no pus is found,
the presence of the parasite causes atrophy of the skin, and at last pit-
like depressions or more extensive reddened scars are left. When the
glandular structures are entirely destroyed, the achorion no longer finds
a suitable nidus, and the disease, at that spot, is at an end.”
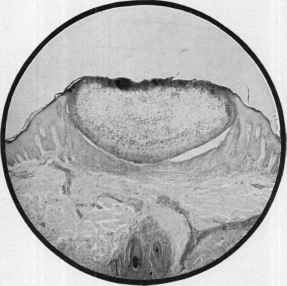
Fig. 274.—Section through a favus scutulum, showing the thinning and atrophy of
the underlying surface, presumably as the result of pressure (courtesy of Dr. M. B.
Hartzell).
While the malady is generally considered to be due to the one variety
of fungus, there is a growing belief that future investigations may show,
as now accepted in ringworm, that there may be several species. On
this basis the variable contagiousness shown and the slight variations in
the clinical features might find satisfactory explanation. Several ob
servers (Quincke, Frank, Unna, Sabrazés, Bodin)2 have found several
varieties. Both Frank and Unna, from experimental inoculations and
1 Darier and Hallé, “Sur un cas de granulome favique,” Annales, 1910, p. 127, state
that the achorion can get down into the living tissue, and rarely may produce kerion-
like lesions and lesions with histopathologic resemblance to tuberculid.
2 Quincke, Monalshefte, 1887, p. 981; Frank, ibid., 1891, vol. xii, p. 255 (with
review); Unna, ibid., 1892, vol. xiv, p. 1; and also in Brit. Jour. Derm., 1892, p. 139
(with colored plate); Sabrazés, “Sur le favus de l’homme, de la poule et du chien,”
Annales, 1893, p. 340; Bodin, loc. cit. (with complete review and references); and “Sur
un nouveau champignon du favus (achorion gypseum),” Annales, 1907, p. 585 (with
review and references).
FAVUS
1101
cultures, conclude that there are three distinct species which give rise
to slightly different clinical pictures. Sabrazé’s experiments and observa
tions indicate that there is one variety peculiar to fowls, one to the dog,
and the other to man, the three being intercommunicable. On the other
hand, other investigators (Elsenberg, Král, Dubreuilh, Danielssen,
Busquet, Mibelli)1 have either failed to confirm such findings or ascribe
the alleged differences to the character of the “soil,” culture methods,
and other accidental or accessory conditions.2 In 200 cases of scalp
favus Sabouraud found them all due to the achorion Schönleinii. The
conclusion seems to be that only exceptionally is the disease due to any
other fungus variety.3
Diagnosis.—The characters of favus—the yellow, and usually
cup-shaped crusts, brittleness and loss of hair, the underlying atrophy,
together with the history—are generally so distinctive that it is, as a
rule, readily recognized. In cases in which the scalp has been thor
oughly washed just before seeking advice the peculiar crusts will be
lacking, but the other features, especially the atrophic or cicatricial
condition of the involved surface, will commonly be sufficient. In such
instances hairs from the affected area can be examined with the micro
scope, or the patient permitted to go and return in a week or ten days,
with instructions that in the meantime no application is to be made or
the parts washed; by the end of this period there is usually a reappearance
of the yellowish points and cup-shaped disks, although the latter may not
have acquired any size. But such beginning crusts can be microscop
ically examined and the matter readily determined. In cases in which
the disease has been long continued the cup-shaped crusts are commonly
wanting, the scalp being more or less covered with irregular, mortar-
like, yellowish, or brownish-yellow accumulations; but the color and
odor of the latter, together with the other characters named, especially
the atrophy and hair loss, afford means for diagnosis. In some in
stances—in those in which, from extraneous matter and the coexistence
of a seborrhea, the crusts are of a less granular character and brownish
in color—there is, on first glance, a possible doubt, but a consideration of
the essential features named suffices to clear the difficulty. In doubtful
cases the microscope is to be resorted to.
The diseases with which it is most likely to be confounded are eczema,
ringworm, seborrhea, and psoriasis. The atrophic and scar-like charac-
1 Elsenberg, Archiv, 1889, p. 179; Král (Pick and Král), ibid., 1891, Ergänzungs-
heft (the fungus described is, however, somewhat different from that commonly found;
gives review and references); Danielssen, Atlas of Vegetable Parasite Diseases, Bergen,
1892; Busquet, Annales, 1892, p. 916; Mibelli, Giorn, ital., 1892, fasc ii, iii—abs. in
Monatshefte, 1893, vol. cvi, p. 47.
2 Of great interest in “this connection also is the observation by Mewborn, Jour.
Cutan. Dis., 1903, p. 11 (with culture illustrations, and résumé of pertinent literature,
with bibliography), of “A Case of Favus of the Scrotum, Coexisting with Ringworm of
the Thigh, Giving Identical Trichophyton-like Cultures” (a megalosporon ectothrix of
probable animal origin).
Winfield, Jour. Cutan. Dis., 1897, p. 13 (with illustration of case and fungus), met
with an instance of a favus-like eruption on the oral mucous membrane (roof of the
mouth), with many points of resemblance in color and crusting to favus, but which was
found due to the aspergillus nigrescens.
3 Four animal species of the fungus are usually acknowledged: achorion Quincke-
anum; achorion gallinæ, oöspora canina, and achorion gypseum.
1102
PARASITIC AFFECTIONS
ter, the condition of the affected hair, the hair loss, the odor and history,
as well as the other features, will serve to distinguish it from eczema,
seborrhea, and psoriasis. In none of these is there a tendency to patchy
hair loss. Ringworm lacks the crusting and atrophic changes of favus,
and ordinarily shows but slight scaliness and a distinct tendency for the
hair to break off, especially near the follicular outlets; moreover, ring
worm patches are likely to be fairly well rounded, while the favus areas
are commonly somewhat irregular (see Ringworm for other differential
points). The atrophic, cicatricial areas of lupus erythematosus occurring
on the scalp show some resemblance, but they lack the crusting and other
features, and the disease is usually seen here in association with charac
teristic patches on the face. Alopecia areata can scarcely be considered,
inasmuch as it has only one feature in common,—the hair loss,—showing
no scaling, crusting, or cicatricial formation.
The diagnosis of favus of the non-hairy or general surface rarely,
if ever, gives rise to difficulty. The ring-shaped patches sometimes
present a similarity to ringworm, but the yellowish points and cup-
shaped crusts of the former are not seen in the latter disease. The
features of favus of the nails are elsewhere considered (see Onycho-
mycosis).
Prognosis.—Favus of the scalp, if at all advanced and of some
duration, is a most intractable disease. In some instances it may, in
deed, be almost said to be incurable; that is, the time required to bring
about permanently favorable results is so long, varying at least from
six months to one or two years, and the measures of treatment so irksome
and tedious that very few patients among the class in which the disease
prevails will be found to be sufficiently persevering. It is true the malady
after years tends gradually to wear itself out, and patients will occa
sionally be seen with the evidences of its ravages, such as atrophic scar
ring and baldness, in whom, after a duration of five, ten, or fifteen years
or more, spontaneous cure has resulted, helped, doubtless, by treatment
pursued irregularly from time to time. In my earlier experience in
dispensary practice I often thought I saw cures resulting after several
months’ treatment, but a larger observation and returning patients have
taught me that while the disease was apparently cured, it was only bene
fited and somewhat diminished in area; and that a permanent and com
plete cure requires a much longer period and the employment of actively
energetic measures of treatment. Under the latter circumstances the
malady in every instance can finally be removed—some cases in five or
six months, but most of them in not less than a year. Efficient depila-
tion, if it can be carried out, has a material influence in shortening the
duration of treatment. Recent and limited cases are, of course, much
more readily responsive, and require less time for their cure; and, more
over, it is true that x-ray treatment (see Ringworm) in skilled hands
has, in some cases, considerably changed the unfavorable outlook.
Favus of the general surface is comparatively easy to cure, and, as
a rule, responds to proper measures in the course of one or two weeks
in the slight limited cases, to one or two months in those of extensive
distribution.
FAVUS
1103
Treatment.—A necessary preliminary in the management of
favus of the scalp is the removal of the crusts, which can be accom
plished by oily applications and soap-and-water washings, the washings
alone often sufficing. An essential part of the treatment is the extrac
tion of the hairs from the diseased areas; the hair of the unaffected
parts should be kept closely cropped, so as to permit of the detection
of any new foci of disease. The most efficient plan of depilation is
by means of the forceps, going over the whole diseased region, taking
a small part each day; it is slow and somewhat painful, and must, more
over, be repeated in many cases two or three times before a cure results.
It is found, however, that the second or third time, if it is required, need
not be so general as the first. The application of a strong carbolic acid
wash just before depilation is practised will lessen the pain of this pro
cedure. If this tedious plan is not feasible, then the hair should be
seized, near the scalp, between the thumb and a spatula or similar flat
instrument and a moderate amount of tractive force used; the diseased
hairs can be thus pulled out, while those sound and firmly seated slip
through. It is not so effective as depilation by the forceps. The use
of a depilatory, as in ringworm of the scalp, from time to time will be found
an efficient substitute for these harsher methods. The x-ray treatment
has some advocates, both for its depilating and curative action, but
should be employed with extreme caution, in the same manner as ring
worm (q. v.); and unless one is experienced in its use, it is much wiser
to hold to the usual plans of treatment.
The whole scalp is to be washed every day with sapo viridis and
hot water, the lather permitted to remain for from five to thirty minutes,
according to the irritability of the skin, and then rinsed off; after the
scalp has been rubbed dry the remedial application is made. These are
essentially the same as employed in the treatment of ringworm of the
scalp. The most valuable are mercuric chlorid, from 1 to 4 grains
(0.065-0.26) to the ounce (32.) of water; sulphurous acid, pure or slightly
diluted; ointments of tar, sulphur, and mercury; pyrogallol ointment,
from ½ to 1 dram (2.-4.) to the ounce (32.); chrysarobin ointment, from
30 to 60 grains (2.-4.) to the ounce (32.). A good compound ointment
is the following:
R. Ac carbolici, 3j (4-);
Ungt. picis liq.,
Ungt. hydrargyri nitrat., ää 3ij (8.);
Ungt. sulphuris, 3iv (16.).
As a certain amount of chemical change takes place in this, it should
be made up fresh about once weekly.
Crocker cured 1 case of twelve years’ duration with an ointment
consisting of 1 dram (4.) of resorcin to the ounce (32.) of lanolin and
oil. If a lotion is selected, it should be rubbed in gently for a few
minutes and then dabbed on for four or five minutes and allowed
to dry in; caution should be exercised in the use of strong lotions
of mercuric chlorid. If an ointment is prescribed, it should be thor
oughly worked into the cutaneous structures by more or less vigorous
1104
PARASITIC AFFECTIONS
rubbing; and, better still, if at bedtime this rubbing in of the ointment is
followed by its application as a plaster spread upon lint or any suitable
material. After a few months’ treatment the remedies should be dis
continued for a time in order that the effect may be properly observed.
In all cases after several months’ active management the malady will
be found to be much less extensive in area, and in resuming therapeutic
measures this should be taken into account, depilation being practised
upon and about the diseased areas only, the hair on other parts of the
scalp being kept short for easy inspection. In this manner, if the treat
ment is energetically pursued and faithfully carried out by the patient
or attendant, the surface involved becomes less and less, and a cure will
sooner or later result. The new-growing hairs in the affected areas
should be examined microscopically from time to time for any evidence
of fungus. If there are no signs of a return of scaliness, yellowish points,
or dulled, lusterless hair in five or six weeks after cessation of treatment,
the case may be considered as cured.
In favus of the general or non-hairy surface the crusts are to be
washed off with soap and water, or by the conjoint application of soften
ing ointments or oils and frequent washings or alkaline baths. This is
usually effected in one or several days. The remedial applications are
ointments of sulphur, 1 or 2 drams (4.-8.) to the ounce (32.); of white
precipitate, from ½ to 1 dram (2.-4.) to the ounce (32.); of mercury oleate
ointment, from 10 to 20 per cent, in strength; of tar, 1 or 2 drams (4.-8.)
to the ounce (32.); of pyrogallic acid, from 20 to 60 grains (1.3-4.) to the
ounce (32.); of chrysarobin, from 10 to 60 grains (0.65-4.) to the ounce
(32.); of resorcin, from ½ to 1 dram (2.-4.) to the ounce (32.); and, in fact,
any of the so-called parasiticidal remedies. Sulphurous acid, diluted
with 1 or 2 parts of water; a 2 to 5 per cent, lotion of carbolic acid, and
painting with tincture of iodin, will also have usually a promptly curative
action. The ointments of mercury oleate and pyrogallol are applicable
only when the disease is of limited extent.
Constitutional treatment is generally considered uncalled for in
this malady, but I am convinced that improvement in the general
health and nutrition is of contributory service, although it may be slight.
Cod-liver oil, in doses of ½ to 1 dram (2.-4.), along with 3 to 10 grains
(0.2-0.65) of sulphur three times daily, have, I believe, some influence;
the former by improving the nutrition, the latter by the resulting cuta
neous sulphurous exhalation, making the skin a less favorable habitat
for the fungus.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |