| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
I. RINGWORM OF THE GENERAL SURFACE
Synonyms.—Tinea circinata; Tinea trichophytina corporis; Trichophytosis corporis;
Ringworm of the body; Ringworm of the non-hairy surface; Ringworm of the glabrous
skin; Fr., Herpès circiné; Herpes circiné parasitaire; Herpès parasitaire; Tricophytie
circinée; Trichophytie des parties glabres; Ger., Herpes tonsurans; Herpes tonsurans
circumscriptus; Scherende Flechte; Tricophytie der unbehaarten Hautstellen.
Symptoms.—Ringworm of the general or non-hairy surface, or
tinea circinata, as it is quite commonly called, may exhibit, as more
especially regards its inflammatory characters, some variations. In

Fig. 275.—Ringworm (tinea circinata) (courtesy of Dr. M. B. Hartzell).
its typical and most common expression the malady presents as one,
several, or more small, slightly elevated, sharply limited, somewhat
scaly, hyperemic spots. They spread in a uniform manner peripher
ally, and as they extend tend to clear up more or less completely in
the central portion, assuming a ring-like aspect. Usually, when coming
under observation, on the average several days to one or two weeks after
their first appearance, the patch or patches are from ½ to 1 inch in di-
1110
PARASITIC AFFECTIONS
ameter, the innermost or central part pale red, or of apparently normal
color, with or without a trifling, often scarcely perceptible, furfuraceous
scaliness; and the outer portion somewhat elevated, but rarely to a
conspicuous degree, hyperemic or mildly inflammatory, and somewhat
scaly. The hyperemia, inflammatory character, and scaliness are sharply
contoured externally, while gradually diminishing on the inner side.
The scaliness is seldom more than moderate in amount; usually it is slight.
After reaching a variable size, from a part of an inch to several inches in
diameter, they remain practically stationary, or in most instances after
a time tend to spontaneous disappearance. After the first several days
or a week, more especially when the spreading tendency has about ceased,
the color often becomes paler, and even goes into a pale, brownish red.
At times, when close together, several may merge and form a large, irreg
ular, gyrate patch. As commonly noted there are rarely more than

Fig. 276.—Ringworm, showing the rather uncommon occurrence of a double ring.
Illustration also shows a marked example of freckles.
several patches present; in some instances only one, in others five to ten
or more.1 In some cases the patches remain small and insignificant,
and with but little, sometimes no, tendency to clearing; in such they
appear to be more of the nature of rounded, brownish-red or brownish-
yellow, scurfy spots, with practically no distinct inflammatory signs,
and lacking the sharply defined border. In others the areas consist of
ill-defined rings, some segments, and some scurfy spots. Very excep
tionally a patch may consist of two or three concentric rings.
The most frequent sites for ringworm are the face, neck, hands, and
forearms, although they are quite frequently seen elsewhere. In rare
instances the palm is the seat of one or two patches, usually quite inflam-
1 Colcott Fox and Blaxall, Brit. Jour. Derm., 1898, p. 37, report two instances in
brothers, aged five and seven, in whom, especially in one (illustration given), the patches
were quite numerous and of somewhat general distribution, but none on the scalp; in
fection probably from a “mangy” cat.
RINGWORM 1111
matory, the ring-like border being of a vesicopapular or papulosquamous
character. The sole of the foot is also a rare site, and here it may appear
as just described, or of its ordinary clinical features; or it may simulate
flattened, callous-like areas; two such cases have come under my observa
tion. In rare instances a patch in the neighborhood of the lips or vulva
has been noted to extend on to the mucous membrane (tinea of the mu
cous membrane).1 In very exceptional examples of the mildly inflam
matory and slightly or moderately scaly type the patches are somewhat
generalized and quite numerous, sometimes with much less tendency to
central clearing than commonly seen, and exemplifying the cases ob
served in Vienna and described under the name of herpes tonsurans
maculosus,2 although most of such cases are, it is believed, examples of
pityriasis rosea.
Instead of the malady appearing as slightly inflammatory maculo-
squamous rings, sometimes the process is of a severer grade; the pe
ripheral portion is observed to be markedly elevated, red, showing a good
deal of inflammatory action, and not infrequently constituted of closely
set papules, vesicopapules, or exceptionally vesicles, which may even
become pustular. It spreads in the same manner and in other ways is
similar, the central portion clearing up; it differs from the common
milder type chiefly in the degree of inflammation. In some of these cases
as the patch spreads the center clears somewhat, but becomes studded
with papulopustules or pustules. In other, rarer, instances the condition,
usually consisting of one or several patches, is over the entire area fairly
uniform in the character of the inflammatory process, with but little,
sometimes scarcely perceptible, lessened activity centrally; the extreme
border is, however, rather more elevated. Such patches, with practically
no disposition to clear centrally, have a decidedly eczematous aspect,
often with considerable infiltration, differing from the latter disease only
in the sharply defined character of the border.
In other rather rare cases (Ojelaleddin-Moukhtar, Whitfield, Sa-
bouraud)3 the malady may show itself on the hands and fingers and also
1 Robinson (case demonstration) and also Cutler (discussion), Jour. Cutan. Dis.,
1893, p. 366, record such instances, extending to the lip and mucous membrane of the
mouth; Giletti (cited by Malcolm Morris, loc. cit., p. 78) has reported a case of pri
mary ringworm of the mucous membrane of this region.
2 I recall clearly an instance of extensive distribution involving the trunk chiefly, in
Professor Neumann’s clinic, when a student of this distinguished teacher, in which the
diagnosis was confirmed by the microscope. Jarisch (Die Hautkrankheiten, Vienna,
1900, p. 580) is right, I believe, in his opinion that there are two maladies which clinic
ally are often indistinguishable—the one, pityriasis rosea, the other, a type of exten
sively distributed ringworm, the latter being rare.
3 We owe our knowledge of these vesicobullous and eczematoid types of the hand,
foot, and toe regions especially to Whitfield, Lancet, July 25, 1908; and Brit. Jour.
Derm., 1911, p. 36, and to Sabouraud, Annales, 1910, p. 289, and Archiv, 1912, cxiii,
p. 923, although in a contribution curiously overlooked, Ojelaleddin-Moukhtar,
Annales, 1892, p. 885, had several years previously directed attention to it. The
etiologic fungus is (with possibly some exceptions) the epidermophyton inguinale; the
same fungus has been found recently to be the usual etiologic one in tinea cruris—
entirely distinct from the ordinary ringworm fungi. The several conditions are fur
ther presented by Whitfield and Sabouraud, and fully discussed by Pringle, Pernet,
Colcott Fox, Adamson, Bunch, Dore, Sequeira, Graham Little, Bolam, Gray, and
Malcolm Morris, in Brit. Jour. Derm., 1911, pp. 375-402. See also paper by Bang,
Annales, 1910, p. 229 (epidermophyton purpureum).
1112
PARASITIC AFFECTIONS
about the feet, especially the toes and interdigital spaces, as a chronic
scaly condition generally diagnosed as “gouty eczema”; or as an acute
vesicular or vesicobullous dermatitis scarcely distinguishable in different
cases from a moderate dermatitis venenata, an acute eczema, or from
pompholyx. In some instances, especially about the fingers, it may pre
sent as ill-defined, somewhat scanty, scattered small vesicles, suggestive
of a mild eczema or extremely mild pompholyx. The vesicular and vesico-
bullous types are rather rare about the feet and toes; in the latter region
it shows itself most frequently about the interspaces and on contiguous
parts, and, as a rule, as an eczematoid eruption, similar to and doubtless
often looked upon as a veritable eczema of these parts. Occasionally it
is more or less strictly limited to one or two interdigital spaces of the
fingers or toes, simulating an inflamed or overtreated moist intertrigo.
Exceptionally in the sole it presents itself in calloused or thickened
epidermic patches or areas. In some instances there will be found
an associated tinea cruris or tinea axillaris, the same fungus (epider-
mophyton inguinale) being etiologic
Another form only rarely noted is that presenting itself as a
somewhat raised, inflammatory patch, beset with crowded follicular
papules or papulopustules, sometimes pustules, and sometimes small
nodular growths. Usually but one or two areas are present, of \ to
2 inches in diameter, and fairly rounded, or irregularly rounded or
ovalish in shape, and showing variable, but generally considerable,
infiltration and depth. It occurs most commonly on the forearm,
back of the hand, and the buttocks, although it may occur on any
part. The hairs of the area drop out, as a rule, but regrowth, after cure,
takes place. In other exceptional instances a similar but still more
advanced inflammatory, deep-seated form is observed, of a somewhat
boggy, pseudocarbuncular aspect, with sometimes considerable elevation,
and a follicular, seropurulent, or mucopurulent discharge; this is a rela
tively moderate counterpart of kerion of the scalp, and also of some of
the boggy tumors of ringworm of the bearded region. This condition
(so-called perifolliculitis suppurative conglomerata) was formerly thought
to be an independent affection (first described by Leloir, Quinquaud
and Pallier, and Besnier and Doyon),1 but is now known to belong among
the manifestations produced by the trichophyton. Very rarely the deep
type extends considerably, the central portion then flattening down,
becoming less active while extension is taking place at the periphery,
where there is a border of deep-seated inflammatory infiltration, with
follicular papulopustules or pustules, so that finally a large, rounded,
or irregularly outlined patch may result (agminate folliculitis) .2 Some
tumor-like lesions of a granulomatous character and aspect (granuloma
1 Leloir, “Sur une variété nouvelle de périfolliculites suppurées et conglomerées en
placards,” Annales, 1884, p. 437; Quinquaud et Pallier, “Des perifolliculites suppurées
agminées en plaques,” These de Paris, 1888; Besnier et Doyon’s French translation of
Kaposi’s Treatise, vol. i, p. 795.
2 See Hartzell’s paper, “A Unique Case of Agminate Folliculitis of Parasitic Origin,"
Jour. Cutan. Dis., 1895, p. 456 (with case illustration and histologic cuts showing the
fungus); Duhring and Hartzell, “A Case of Papulo-ulcerative Follicular Hyphomycetic
Disease of the Skin,” Amer. Jour. Med. Sci., 1895, vol. cix, p. 283.
RINGWORM 1I13
trichophyticum), first described by Majocchi, are exceptionally met with,
sometimes showing ulcerative action.1
One more form remains to be described affecting the genitocrural
region, and known as tinea cruris, eczema marginatum, tinea trichophy-
tina cruris, tinea circinata cruris, epidermophytie inguinale, dhobie itch,
which is more common than the rare varieties just described. It may
begin here, as the ordinary superficial ring type, usually several or more
areas soon presenting, or quite frequently as an intertrigo or a super
ficial intertriginous eczematoid eruption. It may remain somewhat
limited and of a mild to moderate inflammatory grade; or, favored by the
heat and moisture of the parts, the malady develops and may spread
rapidly, the involved areas become more or less uniformly inflammatory
and coalesce. The inflammatory symptoms become predominant, and
the whole of the genitocrural region may be involved, even, in extreme
cases, extending some distance down the thighs, upward on the pubic
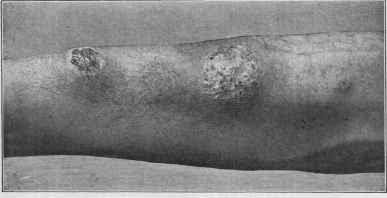
Fig. 277.—Ringworm (tinea circinata) of inflammatory, kerion-like type, consisting
of three patches on forearm; patient a hostler. (The conglomerate pustular folliculitis
of Leloir.)
region, and backward to the anus and immediate neighborhood; in women
it may also extend on to the mucous membrane of the vulva. It then
presents all the symptoms of a moderately or markedly infiltrated true
eczema; the border, however, is somewhat elevated, sharply defined,
and not infrequently,, especially in its earlier existence, one or more
outlying ordinary clinical ring-like or rounded patches of the malady
may be seen. Occasionally this type is also observed in one or both
axillae (tinea axillaris, tinea circinata axillaris), either along with the dis
ease in the genitocrural region or independently. It is not uncommon
1 Schamberg, “A Case of Hyphomycetic Granuloma,” Jour. Cutan. Dis., 1902, p.
410, with case and histologic cuts, review and references; Sequeira, “A Case of Tricho-
phytic Granulomata,” Brit. Jour. Derm., 1912, p. 207, previously briefly reported, ibid.,
1906, p. 269 (a remarkable case of extensive ringworm, especially of the trunk, of years’
duration, with the development of trichophytic granulomata leaving scars, and a per
sistent ulcerative condition of the umbilicus; with brief review of subject (of reports
by Majocchi, Bang, Campana, Pini, Mazza, and Vignolo-Lutati) with references).
Sequeira’s paper and Vignolo-Lutati’s paper, “Ueber Granuloma Trichophyticum Ma-
jocchi,” Monatshefte, 1908, lxvii, p. 184, together give a pretty complete bibliography.
1114
PARASITIC AFFECTIONS
among those who frequent gymnasiums and those engaged in athletic
sports; moderate epidemics occasionally occur among this class. Tinea
cruris (the eczema marginatum of Hebra) had been always thought
due to the ordinary trichophyton fungus, but recent investigations show
the causative fungus to be epidermophyton inguinale.1
Dhobie itch is a name given to this affection (tinea cruris) in certain
tropical countries, where it usually involves both the genitocrural and axil
lary regions; its symptomatology is about the same, except the process is,
as a rule, much more intense in its inflammatory aspects. In the hot
and moist seasons the inflammation from the active proliferation of the
organism and the sweating, heat, and friction of the parts is often so severe
that the patient may be unable to go about, or even to dress. The itch
ing often leads to violent scratching, and the parts may become raw;
and, as a result of secondary bacterial infection, boils and abscesses may

Fig. 278.—Tinea cruris. Ringworm of the genitocrural region.
be added to the ordinary features. On the approach of the cool season
the malady partially and sometimes completely subsides. While it is
usually due to the same organism (Epidermophyton inguinale) as ob
served in the cases of tinea cruris observed here and elsewhere, already
referred to, other parasites, such as the Microsporon furfur, the Micro-
sporon minutissimum, and the organism of impetigo contagiosa (Manson)
have been variously thought to have a bearing in some instances. The
spread of the disease is believed to be by means of the laundry, hence
the name “dhobie (laundrymen’s) itch.”
1 Sabouraud, “Sur l’eczema marginatum de Hebra,” Arch, de med. Experimentale,
1907, Nos. 5 and 6; Alexander, “Beiträge zur Kenntnis der Eczema marginatum,”
Archiv, May, 1912, cxii; Nicolau, “Contribution a l’étude du soi-disant eczema margina-
tum de Hebra,” Annales, Feb. 1913, p. 65 (cases, review of subject with references).
See also references of the eczematoid and vesicobulbous eruptions due to this same
fungus.
RINGWORM
1115
Ringworm of the general surface, as commonly encountered, rarely
gives rise to any troublesome subjective symptoms—occasionally slight
or moderate itching; this, in the more inflammatory types, those which
show an eczematous aspect, and especially when involving the genito-
crural or axillary region, may in some cases be at times quite severe and
troublesome.
Diagnosis.—There is little difnculty in recognizing the ordinary
cases of ringworm of the general surface, as the growth and characters
of the patch, the slight scaliness, the tendency to disappear in the central
portion, together with the history, and, if necessary, by microscopic
examination of the scrapings from the border of the patch. The ring-
like areas of psoriasis bear some resemblance, but it is practically only
in the ring appearance, the other features being wholly different (see
Psoriasis for differential points). The circinate tubercular syphiloderm
has sometimes been confused with ringworm, but the greater infiltration
of the former, its slow course, long duration, color, and often pigmenta
tion, atrophy, ulceration, or scarring generally serve in the differentiation.
Dermatitis seborrhoica, especially as it commonly occurs in the sternal
and interscapular regions, with the segment-like configuration, is some
what suggestive, but the scales of this latter are greasy, and often have
projections into the glandular openings; moreover, these sites are common
for dermatitis seborrhoica, and extremely unusual for ringworm. In
the deep-seated types the markedly inflammatory, follicular, and cir
cumscribed character should always suggest ringworm fungus invasion
and lead to carefully made microscopic examinations. As Hartzell's
case showed, however, sometimes the fungus lies deeply, and must be
looked for in a section of the involved tissue. A circumscribed patch
suggestive of an exceedingly flat, superficial, mild carbuncular formation
should always awaken the suspicion of deep-seated ringworm.
Tinea cruris, and also its counterpart sometimes occurring in the
axillæ, is to be differentiated from eczema and dermatitis seborrhoica of
these regions. The history of the case, its frequent beginning with rings,
its gradual spread and sharply defined elevated border, frequently with
outlying typical ringworm patches, will usually suffice, but in some in
stances careful microscopic examinations of the scrapings from the border
are found necessary for a definite conclusion.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |