| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
II. RINGWORM OF THE SCALP
Synonyms.—Tinea tonsurans; Tinea tondens; Tinea trichophytina capitis; Tri-
chophytosis capitis; Microsporosis capitis; Trichophytia capitis; Trichonosis furfuracea;
Herpes tonsurans; Herpes circinatus; Porrigo furfurans; Fr., Herpès tonsturant;
Teigne tondante; Teigne tonsurante; Trichophytie circinée; Trichophytie du cuir
chevelu; Ger., Scherende Flechte; Herpes tonsurans; Herpes tonsurans capillitii.
Symptoms.—Ringworm of the scalp, or tinea tonsurans, as it is
quite frequently called, in the large number of cases varies but slightly
in its characters, except as to the extent of the involvement. In relatively
few instances, however, the features, one or all, show a material de
parture from the ordinary. It begins usually in the same manner as
that upon the general surface, as a hyperemic, scaly spot, with practically
1116 PARASITIC AFFECTIONS
no tendency to central clearing. In infants or very young children with
light, scanty hair, however, it sometimes presents all the characters
of that on the latter region, showing, moreover, but little disposition,
in the beginning at least, to hair or follicular involvement. Its devel
opment is, as a rule, much more insidious. Sooner or later the hairs and
hair-follicles are invaded by the fungus, and in consequence the hairs
fall out or become brittle and break off, either a little distance from the
skin or just on a level with it. The hyperemia or inflammatory action
is scarcely, and often not at all, recognizable. The surface is a trifle
scaly, rarely conspicuously so. The follicular openings, except in long
standing cases, are slightly elevated and prominent, and the patch may
have a puffed or goose-flesh or plucked-fowl appearance. In other in
stances the surface is somewhat smooth and irregularly scaly, the scali-
ness being of a furfuraceous character, and of a grayish or dirty-gray
color. There may or may not be at times slight or moderate itching, but
it is seldom sufficient to give rise to complaint.
A typical fully developed patch of ringworm of the scalp in the ma
jority of cases is, therefore, noted to be rounded, grayish, somewhat
scaly, and slightly, but often scarcely perceptibly, elevated. The fol
licles, more especially those from which the hairs have fallen, are some
what projecting, usually stuffed with grayish epidermic débris; there
is more or less alopecia, with here and there over the area broken, gnawed-
off-looking hairs, some of which, of a whitish or grayish color, may be
broken off above and just at the outlet of the follicles. Many of the
broken hairs and stumps are surrounded within the follicle mouth and
somewhat above by a powdery sheath, flattening out slightly at the level
of the surface, constituting the so-called circumpilar collarette, which,
when numerous, give the patch a powdery appearance. One, several,
or more such areas, of different sizes from a fraction of an inch to a few
inches in diameter, may be present—in the average case usually two or
three. They extend, as a rule, somewhat slowly, those of the larger
dimensions named requiring several weeks to a few months or longer.
After attaining a variable size, they may remain more or less stationary,
and the malady may thus sluggishly continue indefinitely or new spots
arise here and there. When several patches are in close proximity, from
gradual enlargement coalescence takes place, and a large, irregular area
results. The scaliness rarely consists of more than a slight branniness,
although exceptionally it is of moderate amount. In some children,
after an indefinite duration, sometimes partly as the result of treatment
and sometimes spontaneously, the hairs begin to grow in again, the disease
in great measure disappears, and there are left small scattered spots,
each often scarcely involving more than several follicles, constituting
the disseminated ringworm of Alder Smith. Occasionally the malady
presents itself primarily in this form.
In other instances the inflammatory character is relatively more
pronounced, especially at the periphery, the border consisting of con
tiguous, ill-defined papules or vesicopapules, and in some cases a tendency
to pustulation; the main part of the patch being as already described,
or distinctly hyperemic and inflammatory. In others the whole patch
RINGWORM
1117
may show a scanty or abundant number of papulopustules, and in such
very often, from time to time, considerable crusting may be seen.
The loss of hair of the involved areas is rarely complete, but in most
instances there are no long hairs, those remaining usually having broken
off near the scalp; they are lusterless, brittle, some of them often twisted
up or bent, and which break upon the slightest attempt at traction. In
others most or all of the hairs are broken off just at the follicle mouth,
and give the patch a dotted appearance—so-called black-dot ringworm.
In occasional cases, usually in those of decidedly blonde hair, the hairs
are only moderately lost, not sufficiently so to attract attention, those
remaining being dry, lusterless, often bent and straggly, and easily broken;
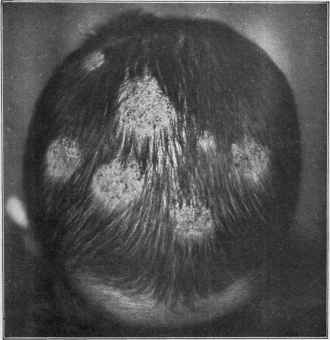
Fig. 279.—Ringworm (tinea tonsurans) of somewhat inflammatory type.
the patch is recognizable only on close inspection, the skin being found
slightly scaly, and sometimes with scarcely perceptible hyperemia. In
exceptional instances, however, the hair loss is not only complete, but it
is rapid, the hairs not breaking off at the surface level, but falling entirely
out of the follicles, the area developing and extending rapidly—consti
tuting the so-called bald ringworm or bald tinea tonsurans of Liveing.
Occasionally a type of ringworm of the scalp, of a markedly inflam
matory nature, known as kerion, tinea kerion, kerion ringworm, de
velops either from a pre-existing patch of ordinary characters or primarily
as such, the inflammation involving the deeper tissues. It presents the
appearance of a more or less bald, rounded, inflammatory, edematous,
boggy, honeycombed, somewhat prominent, carbuncle-like tumor, dis-
1118
PARASITIC AFFECTIONS
charging from the follicular openings a mucoid or mucopurulent secre
tion. It is sometimes painful. If neglected, crusting often takes place,
and the pent-up discharge may undergo change and become offensive.
Those hairs which have not fallen out come away with practically no
traction. If pressure is made laterally, the thick, glairy, mucoid or
mucopurulent secretion can readily be ejected. Very often the intensity
of the inflammatory action results in destruction and dislodgment of
the fungus, and a spontaneous cure results. This type practically cor
responds to the boggy or tumor-like formation frequently seen in ring
worm of the bearded region, and also to that rarely encountered on the
general surface. To a prominently elevated kerion-like type, appearing
as variously sized nodular elevations, and which, instead of discharging
through the follicles, gradually breaks down and empties like an abscess,
Majocchi has given the name of granuloma trichophyticum.1
Diagnosis.—Ringworm of the scalp, as commonly encountered,
presents a clear and decisive symptomatology; its features—the slight
scaliness, broken hair, hair-stumps, the black dots, often prominent
follicles, with more or less baldness of the involved area, together with
the history—are ordinarily sufficiently characteristic to prevent error,
and will serve to exclude such maladies as seborrhea, psoriasis, and
eczema, in which such a symptom-complex is lacking. The hair loss
and nutritional changes in the hair are the most important differential
points. Moreover, the scaliness of psoriasis is more abundant, and
patches are usually to be found elsewhere. Eczema is commonly diffused,
quite itchy, often with considerable scaliness, and frequently with a
history of gummy oozing. Seborrhea is, as a rule, general over the scalp,
the scales are greasy, and while there may be some thinning out of the
hair, this does not occur in patches.
Favus and alopecia areata are the two diseases with which con
fusion is most likely to be experienced. In favus, although the same
tendency to hair loss and the same lusterless and brittle condition of
the hairs are noted, the presence of the yellowish, cup-shaped crusts or
mortar-like accumulations, and the atrophic character of the involved
skin, are wholly different from what obtains in ringworm. Nor are the
patches of favus, as a rule, rounded as they are in ringworm. The
incomplete hair loss, the scaliness, the brittle and broken hairs, and the
hair-stumps will serve to distinguish the malady from alopecia areata,
in which the sole symptom is loss of hair, complete in character, the skin
being perfectly smooth and with a shiny and highly polished appearance.
As between the rare type, bald ringworm, and alopecia areata, micro
scopic examination of the hairs from the edge of the patch will usually,
if the former disease, disclose fungus, and thus serve to distinguish it.
In fact, in all cases of doubt as between ringworm and the several mala
dies named, the microscope should be resorted to. It is to be remem
bered that ringworm of the scalp, with extremely rare exceptions, never
occurs in the adult.
The inflammatory types of ringworm are rare, and while such in-
1 Majocchi, “Granuloma tricofitico,” Boll, della. Accad. Med. di Roma, 1883, and
“Atti dell VII riunione della,” Soc. Ital. di Derm, e Sifil., Milan, Sept., 1906.
RINGWORM
1119
stances resemble some of the inflammatory diseases, especially eczema,
the hair loss and involvement, the history of the case, its limited area,
and, if necessary, microscopic examination, will suffice to differentiate.
Kerion should not be confused with carbuncle; a mistake, strange to say,
that has been occasionally made by surgeons. The boggy, circumscribed
character, the mucoid or mucopurulent discharge from the follicular
openings, and frequently a history of its having begun as an ordinary
ringworm patch are points of difference.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |