| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
TINEA VERSICOLOR 1147
TINEA VERSICOLOR
Synonyms,—Pityriasis versicolor; Chromophytosis; Dermatomycosis furfuracea;
Mycosis microsporina; Chloasma (of older writers); Liver-spots (of older writers);
Fr., Pityriasis versicolore; Gr., Kleienflechte.
Definition.—A vegetable parasitic disease, characterized by vari
ously sized and shaped, furfuraceous, macular patches of a yellowish,
fawn color, and occurring for the most part on the upper portion of the
trunk.
Symptoms.—The disease begins as one or more yellowish or
brownish, macular points, frequently at the follicular outlets (Besnier
and Balzer), and commonly upon the chest anteriorly or posteriorly,
although the earliest spots are sometimes seen lower down or at or near
the axillary folds. Their growth is usually slow, several months or more
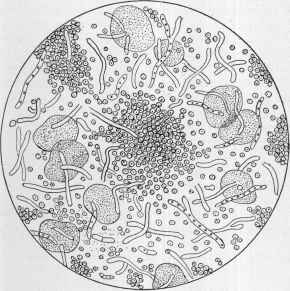
Fig. 304.—Fungus of tinea versicolor—microsporon furfur (X about 500; partly dia
grammatic).
elapsing before the eruption is of conspicuous extent. The beginning
points or spots extend peripherally, and together with other patches
that are present or subsequently arise may finally result, in some in
stances, in an almost continuous sheet of eruption, and involve the
greater part of the upper trunk, often extending lower down. In an
average case this former region is noted to be the seat of variously sized
spots and areas, varying in size from the beginning lesions to large
plaques. There is slight, sometimes scarcely perceptible, furfuraceous
scaliness, less noticeable in those of naturally moist skin or who perspire
easily. The color of the patches is pale yellow or brownish yellow, ex-
1148
PARASITIC AFFECTIONS
ceptionally a yellowish brown; in rare instances, in those of delicate
skin, there may be more or less hyperemia, and in consequence the
eruption is of a pinkish or reddish-yellow tinge, most marked at the edge
of the patches. The eruption is wholly macular, with practically no
elevation; exceptionally, however, there is slight elevation at the follicu-
lar orifices, a faint attempt at follicular papulation.1 Beyond the dis
figurement caused, the disease never gives rise to any trouble, except
that slight or moderate itching, especially when the patient is warm or
perspiring, is frequently complained of.
While in most patients the eruption is practically limited to the
upper half of the trunk, in many instances the whole lower part is also
more or less invaded, and in extreme cases the axillæ, portions of the
arms, flexures of the elbows, and even the genitocrural region and pop
liteal spaces are likewise involved. The eruption exceptionally is noted
to be, for a time at least, more or less limited to the genitocrural region.
Quite frequently it extends from the chest well up on the neck, and in
occasional examples still higher on to the lower part of the chin. It is
generally believed that the face is never the seat of the eruption, but in
occasional instances this has been observed (Biart, Payne, Gottheil,
Allen, Sobel, Powell2), producing chloasma-like patches of diffused dis
coloration, of which one well-marked example has come to my own notice;
it is usually, however, in connection with the eruption extensively de
veloped on the favorite situation. While on the face it is essentially
similar in color to that on the trunk, it may be somewhat darker, or it
may, in the negro, be somewhat lighter, as in Gottheil's case, in which
the spots, doubtless owing to the scaliness, were of a dingy-white, vitiligo-
like aspect. In Biart’s patient the scalp was encroached upon; and in
Payne’s it was both in the bearded and scalp regions, where it appeared
to be a simple furfuraceous scaliness, the scrapings disclosing the fungus.
Both his and Biart’s patient had the eruption on the trunk also. In
my patient, a woman, it had the appearance of an extensive chloasma,
for which, unless closely inspected, it could have been readily mistaken.
1McEwen, “An Unusual Case of Tinea Versicolor,” Jour. Cutan. Dis., Jan., 1911
(with case illustrations), records an instance in which while the eruption was pre
dominantly of the usual clinical type, it presented quite a large number of follicular
papular lesions, giving parts where such lesions were numerous the impression of a
“lichenoid follicular inflammation.”
2 Biart, Jour. Cutan. Dis., 1885, p. 73; Payne, cited by Crocker, Diseases of the
Skin, second ed., p. 892; Gottheil, Med. Record, 1901, vol. lix, p. 649; C. W. Allen,’
Jour. Amer. Med. Assoc, 1901, i, p. 938; Sobel, Philada. Med. Jour., 1901, vol. vii,
p. 1061; Powell, Brit. Jour. Derm., 1900, p. 142, states that it is quite common on the
face in Assam, and the fungus seems identical with that met in Europe, and which
Pernet, to whom scrapings had been sent, demonstrated by examination before the Der-
matological Society of Great Briain and Ireland; Castellani, Brit. Med. Jour., Nov. 11,
1905, and Jour. Trop. Med., 1905, p. 252, states that in Ceylon two types are met with:
tinea versicolor nigra, the eruption being black and lusterless, and found on any part of
the body except the face; and tinea versicolor flava, of which there are two varieties—one
attacking the face, neck, and upper part of the trunk, and the other presenting a lighter
yellow or nearly white patches, generally seen on the arms and legs; it is not uncommon
to see the different types on the same individual. In a later paper (“Tropical Forms of
Pityriasis Versicolor”), Jour. Cutan. Dis., 1908, p. 393 (with 2 case illustrations, fungus,
cuts, etc), Castellani adds another variety, tinea versicolor alba, in which the color is
extremely light, sometimes altogether white; it is oftener seen on the arms and legs than
on the face and chest. These several types, he states, are due to different fungi.
Plate XXXII.

Tinea versicolor, showing the confluent areas and the variously sized patches ; of
several years’ duration. The eruption is not elevated, the chief characteristics being the
fawn or brownish-yellow color, upper trunk distribution, and usually a slight, sometimes
scarcely perceptible, branny or furfuraceous scaliness. In this instance extends well up
the neck and some spots on arms.
TINEA VERSICOL OR 1149
Smith1 met with an instance of its limitation to the soles, and Gottheil2
to one palm, probably the only examples on record.
The course of the disease is slow, and usually progressive up to a
variable extent, and then it remains more or less stationary, showing
little, if any, tendency to spontaneous retrogression.
Etiology and Pathology.—The disease is due to the vegetable
parasite known as the microsporon furfur, discovered by Eichstedt in
1846. Both sexes are liable, but men more frequently. It is rarely seen
before adolescence or in advanced years. While the fungus is abundant,
yet observations show that the malady is but mildly contagious. Not
more than two or three instances of its occurrence in two members of a
family have come under my own notice. Huble3 cites 9 cases of con
tagion from man to wife, or vice versa, and Knowles and Corson,4
in three sisters. Huble and several others have been successful with
inoculation experiments, but, as a rule, success is only occasional. It
is commonly believed, and doubtless true, that those who sweat freely
are its more common subjects. It is thought to be relatively frequent
in phthisical patients,5 but this is probably more apparent than real,
inasmuch as, owing to the exposure of the chest in such patients for the
purpose of physical examination, the eruption is oftener disclosed.
The fungus consists of mycelium and spores, the latter being dis
posed in distinct groups or masses. It is readily demonstrated by plac
ing some scrapings in a little liquor potassæ on a glass slide, and placing
over it the cover-glass, and allowing it to soak for a few minutes; a
power of 200 to 500 diameters gives sufficient amplification. The para
site luxuriates in the corneous layer of the epidermis, sparing the rete,
hairs, and true skin.
Diagnosis.—The color, peculiar characters, and distribution of the
eruption are the diagnostic factors; added to these is the fact that in
most cases coming under observation the malady has already lasted for
a year or more. These points, as well as the large patchy or sheet-like
character usually noted, will serve to distinguish it from the macular
syphiloderm. It can scarcely be confounded with chloasma (q. v.). It
is well to bear in mind, however, that exceptionally the eruption may
invade the face and simulate this latter malady. Occasionally, when in
profusion, the spared skin looks relatively white and might suggest
vitiligo, the fawn color of tinea versicolor being mistaken for the hyper-
pigmented border of vitiligo patches. The inflammatory characters of
1 E. D. Smith, New York Med. Jour., 1896, vol. lxiv, p. 583 (on both soles, ante
riorly, in male adult, of some duration; nowhere else).
2 Gottheil, Med. Record, 1899, vol. lvi, p. 15 (left palm in male adult, of dark
color and some years’ duration; illustration); Campana, Clinica Derm, della Universite
de Rome, 1903, p. 13—abs. in Jour. Cutan. Dis., 1904, p. 55—reports a case in which
tinea versicolor affected the fingers and finger-nails.
3 Huble, Revue méd. de Toulouse, July 15,1886; abs. by Thibiérge in Annales, 1887,
p. 414.
4Knowles and Corson, New York Medical Record, Sept. 30, 1911 (three sisters;
occupied the same bed and used the same towels).
5 Duguet and Héricourt, “Sur la nature mycosique de la tuberculose et sur l'évolu
tion bacillaire du microsporon furfur, son champignon pathogène,” Compt. rend. Acad.
de Sci., Paris, 1886, vol. cii, p. 943, have even alleged that the microsporon furfur is
etiologic in the production of phthisis.
1150
PARASITIC AFFECTIONS
dermatitis seborrhoica, and the inflammatory characters and the acute-
ness of pityriasis rosea, will prevent confusion with these maladies. In
all doubtful cases recourse should be had to microscopic examination.
Prognosis and Treatment.—Tinea versicolor is, as a rule, a
readily curable disease. In some instances the fungus seems to be some
what deeply and firmly seated, extending into the follicles, and such
cases yield more slowly. Unless proper precautions be taken relapses
are not infrequent. A plan of treatment that will be found especially
satisfactory in many cases is that consisting of soap-and-water washings
and the application of a solution of sodium hyposulphite. When the
skin is somewhat irritable, ordinary toilet-soap may be used at least once
daily for the washing, shampooing the parts pretty thoroughly, and rins
ing off and rubbing dry. Immediately afterward the hyposulphite
solution, 1 to 2 drams (4.-8.) to the ounce (32.), is freely rubbed in for a
minute or two and then dabbed on and allowed to dry. The solution
should be applied twice daily. In those of sluggish skin, instead of plain
toilet-soap sapo viridis should be used for the washing; or in obstinate
cases instead of plain sapo viridis the following may be employed with
advantage:
R. Sulphuris præcipitati, 3ij(8.);
Saponis viridis, q. s. ad 3ij (64.).
In other instances a manufactured soap containing sulphur or sulphur
and naphthol will be found efficient. During the treatment the under
wear should be thoroughly baked or boiled or soaked in the hyposulphite
solution. With the treatment outlined carefully carried out a suc
cessful result is almost certain in the course of one to three months.
After the cure is apparently effected a remedial application should be
made once or twice weekly for two or three months, in order to guard
against recurrence. In fact, it is a good plan for those who seem espe
cially liable to recurrences to make a practice of using regularly a medi
cated soap, such as above named, as the body soap. It can be readily
understood that even in apparent cures some deep-seated fungus may
have remained, and if the precautionary measures named are not fol
lowed out, this develops and a relapse follows. Attention to these details
of the management of the disease will do much toward insuring perma
nence of the cure. I have been in the habit also of prescribing a few
grains of sulphur daily internally in this disease, believing that its exhala
tion through the skin makes the tissues a less satisfactory “soil” for the
fungus.
Many remedial applications other than that named will likewise
act satisfactorily, but need not be specifically mentioned, inasmuch
as they are the same as the milder remedies advised in ringworm.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |