| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
2. DISEASES OF THE HAIR AND THE HAIR-FOLLICLES
HYPERTRICHOSIS2
Synonyms.—Hypertrophy of the hair; Superfluous hair; Hairiness; Hirsuties;
Hypertrophia pilorum; Hypertrichiasis; Polytrichia; Trichauxis; Fr.,Poils accidentels.
Definition.—Excessive or abnormal growth of hair, either as
regards region, degree, age, or sex.
Symptoms.—Excessive hair growth may be congenital or ac
quired, and of limited (hypertrichosis partialis) or general (hyper-
trichosis universalis) distribution.
Congenital hypertrichosis may be either partial or general, although
both are rare, the former less so than the latter. In partial cases the
hairiness is usually a part of a pigmented nævus—in fact, such are,
as a rule, examples of hairy nævi. The skin is commonly found pig-
mented, and with a variable amount of connective-tissue growth (see
Nævus pigmentosus). In this variety of congenital cases the lower
part of the trunk, especially over the sacrum, is the most frequent locali
zation.
In universal hypertrichosis the growth on those regions where the
hair is normally more vigorous is the most pronounced. The situations
on which lanugo hair never grows, as, for instance, the palms, soles,
etc, remain free, even in instances of markedly excessive general hairi-
1 Cranston Low, “Fungus Infection of the Finger Nails,” Edinburgh Med. Jour.,
Feb., 1911 (an interesting and valuable contribution—19 cases in three years—16
from trichophyton, 2 favus and 1 unknown fungus).
2 Important literature: Jackson, Diseases of the Hair and Scalp, New York, 1890;
Jackson and McMurtry, Diseases of the Hair, 1912; Beigel, The Human Hair, Lon
don, 1869; Leonard, The Hair, Detroit, 1881.
HYPER TRICHOSIS
965
ness. Usually at birth there is noted a perceptible down, with considerable
hairy growth on the normal localities. In others the downy hairs are
noticed only after some months or a few years. These gradually increase
in size, become more or less uniformly pigmented, and almost invariably
of the same color as the scalp hair. These cases are rare, but quite a
number have been recorded, a few of which have been of the female sex.
The body hairiness is often variable as to degree, but always much more
pronounced than normally, and ordinarily the growth is conspicuous.
The face shows the greatest development of the blemish, being more or
less completely covered. This general hairiness is not only usually
congenital, but there is, as a rule, a hereditary history. Examples of
this condition—the so-called homines pilosi, or hairy people—have
been reported by various observers.1 It is commonly noted that these
general congenital hairy individuals show defective development of
teeth, as is also observed in cases of congenital absence of hair. In
Duhring’s patient, however, the teeth were all present and in good con
dition.
Acquired hypertrichosis, compared to the above-described con
genital cases, is a mild affair, but often most harassing to its subjects,
if of the female sex, and these are the only subjects who come profes
sionally under our notice. Exceptionally, however, instances of general
acquired hirsuties have been observed.2 A variable degree of hairiness
often develops in certain families as adult and advanced age is reached,
but more especially in the male line, although it is not uncommon to see
moderate development on some women, not necessarily the face, but on
the usual downy sites of the covered parts, especially the arms and legs.
These cases, however, rarely seek advice. The examples of acquired
hypertrichosis soliciting professional aid are those observed in young
and middle-aged women, who find the down of the chin, lip, and some
times the sides of the face growing stronger, becoming pigmented, and
thus constituting a positive blemish. Various degrees and varieties are
observed, from that of simple exaggerated down to a conspicuous growth.
In others, more frequently in those of advancing years, there may be
1 Beigel (loc. cit.) refers to several instances of recorded cases (with several illustra
tions), of which the most striking are those of Julia Pastrana and Shwe-Maon (Craw-
ford’s case). Julia Pastrana, a Spanish dancer, not only had a fine beard, but the whole
body was hairy, and a daughter displayed the same anomaly. Shwe-Maon, one of his
daughters, and one of her sons, all displayed universal hairiness, the body hairs of his
daughter being, however, chiefly of a downy character. The Russian dog-faced man,
Andrian Jeftichjew, whose picture is now well known, and his son, Fedor, both of whom
were on exhibition in this country and elsewhere, are additional examples. Duhring
(Arch. Derm., 1877, p. 193, with illustration) had under observation a “bearded woman,”
aged twenty-three, in whom there was full growth, such as seen in men, and also more or
less general hypertrichosis, with, however, some parts entirely free. There was no
hereditary history, nor did either of her two children up to the time of their death—at
the ages of two and four—display this tendency.
2 Erasmus Wilson (Lectures on Dermatology, London, 1878) refers to an unmarried
woman, aged thirty-three, in whom general hairiness began to develop at puberty, and
covered the surface, excepting a bald plaque on the vertex of scalp; the woman was a
sufferer from amenorrhea. Zarubin (Jour. Cutan. Dis., 1897, p. 74) records a some
what similar case, in a married woman, appearing at the age of twenty-three, after a mis
carriage with her second child and consequent pain (amenorrhea) in the sexual sphere,
the menses not appearing again for eleven years; the general hair growth was followed
by scalp baldness.
966 DISEASES OF THE APPENDAGES
simply a small number of large scattered hairs or one or two tufts. The
growth of these latter is somewhat akin to the growth of hairs usually
observed in old men about the nasal, aural, and brow regions. In ex
ceptional instances (transitory hypertrichosis) acquired hair growth on
a woman’s face has been noted to disappear spontaneously; this has been
more especially observed to occur after pregnancy or after the re-estab
lishment of normal menstrual flow, following prolonged amenorrhea.1
The hair growth occasionally seen following local injuries, such as frac
tures, nerve traumatism, and the like, sometimes falls out subsequently.
The tendency to excessive growth of the beard in men, and of the
scalp hair to extreme luxuriance and length in some women, is a matter
of occasional observation. This by no means, especially in women,
indicates an excessive production on the other natural situations. In
rare instances the hairy development on parts other than the scalp
takes place early—before puberty, its normal time for active growth—
and has resulted in whiskered boys, associated with early develop
ment of the pubic hairs, or female children with precociously hairy
pudenda.2
In connection with hypertrichosis, the anomaly exceptionally ob
served, two hairs (Giovannini)3 and even three hairs (Flemming)4
emerging from a single follicle, usually on the bearded parts, may be
referred to. One is commonly abortive, although they may be equally
developed and thick. Giovannini is inclined to believe, from an instance
observed by him, that this may give rise to a sycosiform inflammation.
I have myself observed in a few cases in isolated follicles the growth of
two hairs, but never with coincident inflammation. Doubtless in some
instances these double and triple hairs are simply examples of hair-
splitting.
The hair has certain normal directions in which it grows, but ex
ceptionally this may be deviated from. The most frequent example
of this is with the eyelashes, which may tend inward against the eyeball
(trichiasis) and give rise to considerable irritation, and sometimes
opacity of the cornea, etc. In rare instances are observed in this region
two rows of lashes (distichiasis), a supplementary inner row curved back
ward on to the eye, which may extend along the whole lid, but usually
only along the outer third of the upper lid. Both trichiasis and distichia-
sis may result from chronic inflammation of the lid-borders; the latter
1 Gottheil has cited an instance, which was also observed by Jackson (Jackson,
Morrow’s System, vol. iii (Dermatology), p. 841), in which a woman, after having borne
several children, was the subject of a persistent amenorrhea, during which time a growth
of coarse hair grew on the face; several years later she became pregnant, and, after the
birth of the child, the remaining hairs—some had been removed by electrolysis—sponta
neously disappeared.
2 Lesser (Correspondenzbl. f. Schweitzer Aerzte, xxvi, p. 355; Jour. Cutan. Dis.,
1897, p. 75) cites an instance of a girl of six in whom extensive hair growth began at
the age of four, the child developing precociously and menstruating when three years
old. In addition to the natural situations there was, however, also growth on face and
general body surface (an illustration of this case in Lesser’s Hautkrankheiten, tenth edit.,
1900, p. 220); Beigel (Virchow`s Archiv, 1868, vol. xliv, p. 418) also recorded a six-
year-old girl with mature pudendal development; and Chowne (Lancet, 1852, i, p.
421) a boy aged eight, with pubic hairs and a bearded face.
3 Giovannini, Archiv, 1893, vol. xxv, p. 187 (with cuts).
4 Flemming, Monatshefte, 1883, p. 163.
HYPER TRICHOSIS
967
is, however, sometimes congenital or develops about the age of puberty
(de Schweinitz).
Etiology.—Some of the possible causative factors have been
already incidentally alluded to. The condition may be congenital in
a few instances, and in many a hereditary factor is recognizable. Cer
tain races are more especially prone to strong, coarse, and more than the
usual quantity of lanugo growth, with a tendency to become stronger
and coarser. Those of dark complexion are more susceptible. It is
true, too, that masculine women are frequently the subjects of this blem
ish, but such individuals are not very sensitive concerning it and rarely
seek advice, so that, according to my experience, the large majority of
women coming under actual notice for treatment are in nowise less
womanly than those free from facial hirsuties. In fact, I should say
that most of my patients have been exceedingly sensitive, refined, frail,
and womanly. In the larger number of cases the growth develops most
actively at the climacteric period. It is a common observation that the
growth is frequently associated with diseases, functional or organic, of
the utero-ovarian system. On the other hand, in many instances there
is no apparent cause. It is known that local irritation, as the warmth
of fracture dressings, sinapisms, stimulating embrocations, and the like,
are quite capable in some subjects of stimulating hairy development.
There is a strong belief among women that greasy applications to the face
favor hirsutial growth, especially the petroleum ointments, but unless
there is an underlying tendency I cannot, from my own observations,
think this to be true. Friction and petroleum ointment conjointly
might in such subjects have a stimulating influence; but grease of any
kind, even with active friction or massage, is often enough, as we unfortu
nately know, powerless to stay falling hair or to stimulate new growth.
The nervous system is probably a factor in some instances; it is not in
frequent in insane women, although often in association with menstrual
irregularity or abeyance.1
Treatment.—There is no treatment for general hypertrichosis.
For cases of moderate acquired facial hair growth occurring on women’s
faces, and for which relief is often urgently sought, full and permanent
removal can be effected by electrolysis, a dermatologic procedure the
profession owes to Hardaway, who was led to employ it by Michel, who
had been successfully using it for the removal of ingrowing eyelashes.
Since then Fox, Jackson, Brocq, and others have gone over the details
and reported results. The operation is permanent in its effects, but as
each hair must be treated individually, it is only practicable in cases
in which the hairs are coarse and not too numerous. Owing to the deli
cate character of the operation, it is natural that a proportion of failures
—failure to strike the hair-papilla—should occur; and this experience
proves. With a good operator, however, there should not be more than
2 or 3 papillae missed out of 10. The position of the papilla is usually
indicated by the direction of the hair-shaft, but this is not always so,
especially under the chin; the proportion of failures in the latter region
1 H. C. Baum, Jour. Amer. Med. Assoc, July 13,1912, p. 104, thinks that in general
toxic influences are of some import, and indican in the urine bears a relationship.
968 DISEASES OF THE APPENDAGES
is therefore greatest. The surface can be gone over a second time,
however, and complete removal thus attained. I have always declined
to operate on lanugo growth, and have always discouraged the treatment
in extensive cases, as in the former the hair is not conspicuously unsightly,
and it is possible, just at such time, the operation, by producing irritation,
might stimulate the hair; and in the latter the method seems interminable.
From about 35 to 50 hairs can be comfortably operated on in an hour.
Even in extensive growth, however, if the subject have persistence,
patience, and a full purse, a final favorable result can be brought about.
The procedure is somewhat painful, variable as to degree in different
individuals, but it is never an obstacle, for the patient is extremely rare
who cannot sit and bear the slight pain of the operation much longer than
the physician can comfortably operate. The upper lip, especially under
the nose, is the most sensitive part. Anodyne applications, usually
without effect, need not, therefore, ever be used. A good light is re
quired, for at the best the procedure is trying on the operator’s eyes.
The patient can be placed on an ordinary chair with a headrest, or a
reclining chair can be used—it is most convenient for the physician, who
sits at the side facing the patient, when the part to be depilated is on a
level with his eyes.
The object of the electrolytic operation is to destroy the papilla and
lower part of the follicle. For this purpose are needed a galvanic bat
tery of 10 to 30 cells, a needle-holder, an extremely fine needle, the
ordinary cords, an electrode, a rheostat, and a milliampèremeter. The
strength of current required is from ¼ to 1½ milliampères, probably f of
a milliampère being the average. If no meter is used, a current of from
2 to 6 freshly charged cells of a zinc-carbon battery with electropoion
fluid, or from 4 to 10 Leclanché cells, or from the same number of the or
dinary commercial dry cells, or from 8 to 16 silver chlorid cells will give
the required strength; it is better, however, to have a large number of
cells, so that the requisite current can be obtained for some months, as
the cells gradually weaken. Moreover, the battery is then available
for electrolytic and other purposes which require stronger currents.
The needle may be either one of iridoplatinum, suggested by Hardaway,
and which I prefer, or a fine steel one. Fox and Jackson both use a
jeweler’s steel broach. The iridoplatinum needle can be bent in any
direction, a convenience when operating in certain regions. The needle-
holder should not have an interrupter, although, strange to say, more of
these are sold, the general practitioner being the purchaser. The expert
buys the one without, as the current should be broken at the positive
electrode, and not at the needle—the abrupt breakage by the latter
giving rise to flashes, and often giddiness. The holder, with the needle,
is to be attached to the negative pole. If attached to the positive pole, the
needle glues itself slightly in the follicle, and if a steel needle is used, its
oxidation, which takes place at this pole, results in a deposit of iron rust
in the skin. While a milliamperemeter is not an absolute necessity, its
employment is a guard against the use of a too strong current and
therefore lessens the risk of scarring.
The region to be operated upon should be wiped off with a pledget
HYPER TRICHOSIS
969
of cotton wet with alcohol, as a mild preliminary antiseptic measure
which, I believe, lessens the chance of pustulation. For the operation
good light is required; a magnifying lens or a pair of slightly magnifying
spectacles will be a help. The needle is introduced into the hair-follicle
alongside of the hair, down to the papilla; if the follicle is entered, the
needle slips in very readily without puncturing the skin or bringing
blood. The depth to which the needle is introduced depends upon the
individual case and the individual hair, varying from 1/16 to ¼ of an inch;
the sense of resistance met with will usually indicate the proper depth.
The circuit is then made by the patient touching the positive electrode,
which is covered with wet sponge or wet cotton, with the fingers or palm,
the other hand holding this electrode by an insulated needle; the current
is allowed to act for from ten to thirty seconds, during which time the
needle is to be moved a trifle, so as to bring it in contact with the sides
of the lower part of the follicle. Slight blanching and frothing or bub
bling at the point of entrance are noticed while the current is passing.
When sufncient action is thought to have taken place, usually in from
ten to thirty seconds, the patient removes the hand from the positive
pole and the needle is withdrawn. If the papilla has been destroyed,
the hair will readily come out with but little, if any, traction. In many
instances a small, hive-like spot marks the site of each operation, sub
siding in the course of some minutes or hours; in other instances the
reaction is extremely slight. If the action has been too severe or the cur
rent too long continued, and even under the most favorable conditions
in some skins, there is considerable reaction at each of the points of
operation, and pustulation and crusting result in one or two days, with
sometimes slight or insignificant scarring. As a rule, however, if the
operator is practised, careful, and skilful, scarring, in the popular sense
of the word, should not take place. There will be less danger of this if
the hairs operated upon at the one sitting are not too close together—
picking them out here and there, and avoiding closely contiguous hairs.
In fact, operating at the one sitting on adjoining follicles is almost sure
to produce fusing zones of redness or inflammation, and sometimes posi
tive tissue destruction and scarring. Another precaution is not to re-
enter the same follicle at the same sitting—a temptation when the first
introduction has not been successful. On the upper lip the weakest
possible current should ordinarily be used, both on account of the ex
treme sensitiveness of the part and the greater tendency to tissue de
struction. In 2 instances freckle-like pigment spots marked the sites
of operation on the upper lip—1 case of my own and in 1 operated
on by another physician. Jackson also refers to this possibility—an
extremely rare one, however; several weeks or months elapsed before
their entire disappearance. The weaker the current, the less chance of too
much action, although the needle must be kept in the follicle somewhat
longer. After the sitting the part should again be wiped off with alcohol.
Two or three times during the next ten or twelve hours the patient is to
apply hot water for several minutes; this will reduce any reddening or
inflammatory tendency. If there is much reaction, an occasional anoint
ing with cold cream containing 2 or 3 per cent, of boric acid will be of
97o
DISEASES OF THE APPENDAGES
service. The frequency of the sittings will depend upon the amount of
surface involved—if limited, a week is allowed to go by before operating
again; this will have given ample time for all irritation to subside; if the
region is large, sittings can follow closely one after another, a new part or
scattered hairs being operated on each time.
Another method which has recently been experimentally tried is
that by the x-ray. It has been known for some time that its use was
occasionally followed by falling of the hair. Schiff and Freund,1 Wood,2
Pusey,3 and a few others have utilized this fact in treating hypertrichosis,
and with alleged favorable effects, but numerous exposures are required,
and the results can scarcely be said to have been permanent, and it is
not without some risk of troublesome dermatitis and of subsequent
atrophic changes in the skin. Even its former warmest supporters now
recognize its shortcomings. It should be limited, if used at all, to cases
not otherwise manageable, and the exposure be at first cautiously given;
a number of exposures are required. After some months the hair usu
ally regrows, but, as a rule, in less number. It is to be considered an
uncertain and dangerous method.
Although electrolysis constitutes the only method of treatment
that will yield permanent results, there are several other expedients
adopted in such cases which, although only temporary in their effect,
can, by repetition, keep the face free from this blemish. These are ex
traction of the hairs with the tweezers, cutting or shaving, and the
use of depilatories. Another method not so commonly used, but which
I have found occasionally employed, is that by a smooth piece of pumice-
stone; by gently rubbing this over the part every few days the hairs are
kept ground off even with the skin. It is popularly believed, and it is
probably true, that all these methods tend to make the hair stronger
and to promote the growth of the downy hairs. It is even possible that
the operation of electrolysis may have this influence on the remaining
lanugo hairs. Still, when the latter operation is not available, owing to
the necessary expense, time outlay, or other reason, some other expedient
is resorted to. For this purpose depilatories are most frequently em
ployed, and, judging by the extensive advertisement of secret prepara
tions of this character, their use must be quite general. One of the best
depilatories (Duhring) consists of from 2 to 4 drams (8.-16.) of barium
sulphid, with enough zinc oxid and starch to make an ounce (32.).
The sulphid should be well and usually freshly made, and kept tightly
corked, otherwise its action is unsatisfactory. At the time of applica
tion sufficient water is added to make a paste, which is thickly spread
over the part, and allowed to remain for a short time, rarely more than
a minute or two, and then scraped or washed off, and a little soothing
ointment or a dusting-powder applied. A variable amount of redness
follows; the object is to allow the paste to remain on only a sufficient
length of time to destroy the hair, so as to limit the resulting irritation.
1 Schiff and Freund, Wiener med. Wochenschr., 1898, pp. 1058, 1118, and 1178; and
(Freund) Weiner klin. Wochenschr., 1899, p. 966.
2 Wood, Lancet, 1900, i, p. 231.
3 Pusey, Trans. Amer. Derm. Assoc. for 1901.
HYPER TRICHOSIS
971
Ordinarily a feeling of warmth or slight burning is an indication that the
paste has been on long enough. The application is repeated as soon as
the hair has reappeared—about every one or two weeks. Böttger’s
paste, as advocated by Kaposi and Brayton,1 made by passing hydrogen
sulphid into hydrated lime, is also, when well made, a good preparation;
it is to be made into a paste at the time of application by the addition of
water. Brayton2 also commends highly a similar one (dry calcium
sulphohydrate), made by heating together at a high temperature plaster
of Paris and granulated wood-charcoal, although the product, like most
others in my own experience, seems to vary in efficiency. It is also to be
made into a paste at time of application.
In cases in which these various expedients do not seem advisable
or eligible, the bleaching properties of hydrogen peroxid, especially
in patients with a dark growth, can be made use of, as suggested by
Bulkley3 at first, in order to avoid the possibility of irritation, diluting
with an equal part of water, and gradually increasing. It is to be thor
oughly and frequently applied. Bulkley states that it also has the ad
vantage, if constantly employed, of retarding the growth. I can testify
as to its value as a bleacher, and thus occasionally serviceable as a pal
liative, but I have seen no evidence of its retarding influence on the
hair growth.
Plica polonica is a term formerly much in use, applied to a condition
of the scalp hair, especially observed in Poles, in which entangling and
matting were the conspicuous characters. Much was formerly written
upon the subject, several varieties and stages were described, and it
was even deemed worthy of atlas illustration, but all its interest faded
away when it was demonstrated (Hebra), and finally accepted after
much controversial discussions, that it was not in itself a disease, but
simply the result of lack of cleanliness and care, associated with pediculi,
eczematous oozing, and extraneous dirt. Under such circumstances it
can be understood how inextricable matting could readily ensue.
Plica neuropathica is an idiopathic matted or felted condition of the
scalp hair of which but several cases have been recorded—1 by Le Page,4
by Pestonji,5 De Amicis,6 1 by myself,7 and possibly a few others. In
the first 2—young women—the matting developed shortly after washing
the hair in warm water, and in 1 (Le Page’s) was confined to the hair of
the right side, and in the other to the sides of the occipital region. These
cases were, therefore, of sudden development, and though suspicious as
to possibility of artificial production, this element seems to have been
carefully eliminated. In De Amicis’ case, the patient having lost the hair
of the scalp in consequence of typhoid fever, the regrowth on the ante
rior portion was of a bushy, tangled nature, wholly different from the
1 Brayton. Indiana Med. Jour., June and Aug., 1896.
2 Brayton, Jour. Amer. Med. Assoc, April 16, 1898.
3 Bulkley, Jour. Amer. Med. Assoc, 1899, 11, P. 1598.
4Le Page, Brit. Med. Jour., 1884, i, p. 160.
5 Pestonji, Lancet, 1885, ii, p. 431.
6De Amicis, Trans. Internat. Derm. Cong., Vienna, 1892, p. 422; abs. in Annales,
1892, p. 1182.
7 Stelwagon, Amer. Jour. Med. Sci., Dec, 1892.
972
DISEASES OF THE APPENDAGES
other hair posteriorly. This patient had distinct nervous symptoms as
well, leading De Amicis to believe that the condition was a trophoneurotic
one. In my own case the felting was limited to a dollar-sized area poste
riorly just below the occipital protuberance, and had been a growth
of years, forming a rounded, matted, felted lock 4 feet long. The
patient was perfectly cleanly, and the scalp free from dirt or vermin.
The other hair exhibited no tendency to similar felting. It is difficult
to find an explanation of these cases. In the discussion on my own case
White1 suggested that it might be due to some peculiar arrangement of
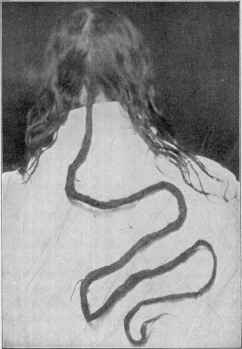
Fig. 243.—Plica neuropathica (case referred to in the text).
the cortical cells, similar to those of the hair of animals in which natural
felting occurs. Unfortunately, my patient was thoroughly imbued with
the superstitious sentiment always associated with these formations, and
I was therefore not able to cut off any for investigation. That excep
tionally a curly or other property can be given to one or two locks or a
part of the scalp hair without necessarily to the whole region uniformly
is also shown by Flesch’s case,2 a boy of six years, in whom were two
locks, of about 1 inch diameter, distinctly curly and light yellow in
color, the other hair being smooth, straight, and brown. No other
member of the family presented this peculiarity, nor was there any
hereditary history of such.
1 J. C. White, Trans. Amer. Derm. Assoc. for 1892.
2 Flesch, Verhandl. Berlin. Anthropolog. Gesellsch., April, 1886; abs. in Monats-
hefte, 1886, p. 522. .
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |