| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
1014
DISEASES OF THE APPENDAGES
SYCOSIS VULGARIS
Synonyms.—Sycosis; Non-parasitic sycosis; Folliculitis barbæ; Sycosis cocco-
genica; Acne mentagra; Mentagra; Fr. Sycosis non-parasitaire; Ger. Bartfinne.
Definition.—A chronic inflammatory affection of the hair-fol-
licles of the bearded and mustache regions, due to microbic infection.
As the disease is now known to be microbic, the term non-parasitic,
formerly used to distinguish it from parasitic sycosis or sycosis due to
the ringworm fungus, is no longer applicable.
Symptoms.—The disease may involve only a part of the hairy
region of the face, as, for instance, a portion of the upper lip, especially
just under the nasal orifices, or the entire mustache region; or it may be
more or less limited to the chin or cover the bearded sides of the face;
finally, in extensive cases, the whole surface covered by the mustache
and beard may be involved, and in extreme instances even the eyebrows
also are the seat of the lesions. In my experience the bearded part and
the mustache have appeared of about equal frequency in being the sites
of the eruption. The disease begins, as a rule, slowly, with the appear-

Fig. 253.—Sycosis vulgaris, limited to region immediately under the nose, usually with
a nasal catarrh as the etiologic factor.
ance of a variable number of small red papules or papulopustules or tu
bercles, the most of which, or all, soon become pustular; each lesion is
pierced by a hair. The pustules are small, rounded, or acuminated and
yellowish in color, with but little tendency to spontaneous rupture.
Exceptionally they may remain for the most part papular. At first
they may be quite discrete, later, from the accession of the new lesions,
the affected part becomes quite crowded, and the inflammation is then
usually confluent, with some infiltration and swelling, and beset with
the numerous, small, projecting lesions. At first the hairs remain firmly
seated, but in most cases in the follicles which undergo more pronounced
suppurative action, they loosen and can be readily extracted; and some
follicles may suffer complete destruction. As a rule, however, in spite
of the rather violent aspect of the disease, but comparatively few hairs
are lost, and positive scarring rarely results. When so closely aggregated
that it practically amounts to coalescence, a portion or the entire region
may become crusted, under which there may be a slight tendency to
fungate. There is often a good deal of infiltration and thickening, and
the parts are of a bright or dark-red color, depending upon the type of
SYCOSIS VUIGARIS
1015
inflammatory action. There is, however, no distinct lumpiness or large
cutaneous swellings as in tinea sycosis (ringworm sycosis).
The lesions in some cases, for a time at least, may remain more
or less discrete, and the area of disease may be limited to two or three
small patches; in most instances, however, new lesions arise, form new
aggregations, and, by still further accessions, the areas become confluent
and a large region is involved. The disease may remain somewhat lim
ited, or it may go slowly from worse to worse, involving more and more
of the hairy parts. While it is essentially chronic, the inflammatory
action being of a subacute or sluggish character with sometimes slight
remissions, there are often acute exacerbations.
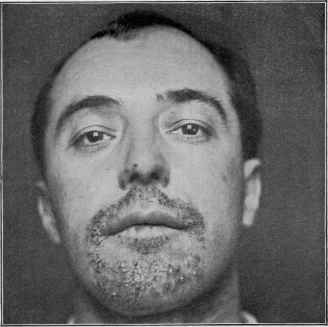
Fig. 254.—Sycosis vulgaris of moderate development, involving chin and to a slight
extent upper lip.
The subjective symptoms are rarely marked or troublesome: there
may be a variable degree of pain and itching and a sense of burning.
In rare instances the disease is limited to the outer portions of the
bearded region, beginning with all the appearances of an ordinary case;
as the process advances it leaves behind a smooth, furrowed, or keloidal
scar, total destruction of the hair-follicles, and permanent loss of hair.
It usually advances in one direction, and, as a rule, with a slightly in
filtrated border. This variety or aberrant form has variously been con
sidered a distinct affection, called lupoid sycosis (Milton), sycosis lupoide
(Brocq), and, finally, and more fully described by Unna,1 under the name
ulerythema sycosiforme.
1 Unna, “Ueber Ulerythema sycosiforme,” Monatshefte, 1889, vol. ix, p. 134.
10l6 DISEASES OF THE APPENDAGES
While sycosis is a disease of the bearded and mustache regions,
and is so understood when the term is used, in exceptional instances
other hairy parts of the body are the seat of similar follicular erup
tion which stops short at the hairy borders; when such occurs, it is, as
a rule, in connection with eczematous eruption elsewhere.
Etiology.—The essential factor of sycosis is microbic; as Bock-
hart1 has demonstrated, the pyogenic cocci (Staphylococcus aureus
and albus) are the usual causative agents, and hence the names sug
gested, sycosis coccogenica, sycosis staphylogenes. In one instance,
presenting the symptoms of ordinary sycosis, Tommasoli2 found that
instead of the usual micro-organisms, a bacillus was the morbific agents
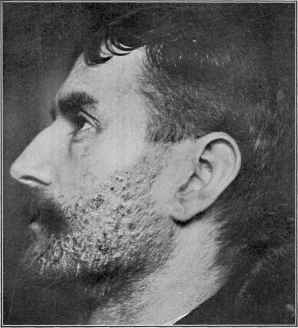
Fig 255-—Sycosis vulgaris, of several years’ duration; involving the entire bearded
region.
and he succeeded, with pure cultures, experimentally in proving this on
himself and rabbits; this discovery led to the variety designation sycosis
bacillogenes.
Accepting the microbic origin, it should be, and indeed probably is
somewhat, though feebly, contagious, although it has never been gen
erally so considered. I have occasionally met with instances in which
the barbershop has apparently been the starting-point, and Brooke3
and others have given evidence of its contagious character. The disease
is, as to be inferred, met with in males only, and usually in those between
1 Bockhart, “Ueber die Aetiologie und Therapie der Impetigo, des Furunkels, und
der Sycosis,” ibid., 1887, vol. vi, p. 450.
2 Tommasoli, “Ueber bacillogene Sykosis,” ibid., 1889, vol. viii, p. 483.
3 Brooke, “The Contagious Nature of Sycosis,” Brit. Jour. Derm., 1889, p. 467.
SYCOSIS VULGARIS
1017
the ages of twenty and fifty. It is not frequent. It is observed in all
walks of life, but is more common among the poor, and especially in those
whose health is impaired. In many cases, it is true, the patients seem in
good condition. Any constitutional disturbance, such as gout, rheuma
tism, dyspepsia, etc, may be of contributory influence.
Local irritation is sometimes of etiologic importance. On the upper
lip, especially the subnasal region, it is often due to the secretion from
a nasal catarrh. Seborrhea is also at times a factor, and occasionally
the disease is observed to follow an eczema of the face. Shaving has been
suggested as a factor, but inasmuch as this procedure is often a necessary
part in the cure of the malady, it can scarcely be considered etiologic
Jackson1 has observed that those whose occupation is in close dusty
rooms, and those in a poor condition of health, furnish the largest number
of cases. The disease has its seat essentially upon the bearded and mus
tache regions, but occasionally the eyebrows share in the eruption. I
have met with one instance in which the scalp and hair-follicles of the
forearms and dorsal surfaces of the fingers were all involved, presenting
the exact symptomatology of the disease as observed on its usual site—
follicular, and stopping at the edge of the hairy skin; this was typically
• shown on the backs of the hands and fingers, intervening hairless parts
being entirely free. The cause of ulerythema sycosiforme is not known—
probably an ordinary sycosis with an added infective factor.
Pathology.—The micro-organisms gaining access give rise to
the inflammatory changes and the clinical manifestations. It can be
readily understood how the process, starting at one point, can soon
involve neighboring follicles by continuous and repeated inoculation.
Tommasoli’s findings indicate that there may be other organisms than
the usual pyogenic cocci. The pathology and pathologic anatomy
have been especially studied by Wertheim,2 Robinson,3 and Unna,4
whose conclusions, while at variance in minute details, are, in their
essential characters, the same. The disease is primarily a perifollicu-
litis, the follicles and their sheath becoming rapidly involved secondarily
in the inflammatory process. The changes are such as are ordinarily
observed in vascular tissue inflammation resulting from these organisms.
The hair-papilla is, as a rule, not destroyed, so that hair loss, except in
very chronic and markedly suppurative cases, does not commonly occur.
The resulting pus escapes at the hair-follicle opening, or through the epi
dermis immediately adjacent. Cocci are usually to be seen in abundance.
As Wertheim states, each follicle really becomes a minute abscess. In
ulerythema sycosiforme the hair-follicles and hair-papillæ, the glandular
structures, and the connective tissue are destroyed and give place to
scar tissue.
Diagnosis.—The disease is to be differentiated from eczema,
which it sometimes resembles, and with which, by some authors, it is
thought to be identical. Eczema rarely stops at the border of the hairy
1 Jackson, “Sycosis: A Clinical Study,” Jour. Cutan. Dis., 1889, p. 13.
2 Wertheim, Wiener med. Jahrb., 1861, ii, p. 87.
3 Robinson, N. F. Med. Jour., Aug. and Sept., 1877, and Manual of Dermatology.
4 Unna, Histopathology.
1018
DISEASES OF THE APPENDAGES
region, and the lesions are, with some exceptions, not pierced by hairs;
eczema is apt to involve the entire skin of the affected area, the follicular
implication being secondary: sycosis involves the follicles primarily,
and only later, when closely aggregated, does the inflammation present
a diffused character. When the latter is present and the parts are
crusted, it is usually necessary to remove the crusts and sometimes
allow a few days to intervene before the case is clear; but in sycosis the
follicular involvement becomes again perceptible. Eczema itches,
usually intensely: sycosis rarely does to any degree. A history of chron-
icity, with no tendency to overstep the borderline, and with but little
variability, would point to sycosis.
Tinea sycosis can scarcely be confounded in average or severe cases;
it begins usually as one or several rings, and continues so, with breaking
of the hair, and often their easy extraction; or it begins in this manner,
or as several lumpy nodules, and rapidly invades the subcutaneous
tissues, and then presents large, nodular swellings, on which the hair
may be broken, fall out, or can be readily extracted. Such conditions
are entirely different from the beginning and behavior of sycosis. In
obscure cases the microscope would decide (see Ringworm).
In acne the evident involvement of the sebaceous glands, the scat
tered lesions, as a rule over the face, evolution, and course, with usually
the presence of blackheads, will prevent its being mistaken for sycosis.
Only carelessness could lead to confusion with a syphilitic eruption;
early eruptions of syphilis are generalized, with other corroborative
symptoms, and late syphilodermata are limited, and usually serpiginous
or segmental in outline.
Prognosis.—The disease is obstinate and persistent, with no
tendency to spontaneous disappearance. The duration, extent, and
character of the inflammatory process must all be considered. Under
proper treatment, however, recovery takes place, in moderately devel
oped cases, sometimes within two or three months, but frequently
longer. In extensive involvement the duration of treatment may be
but several months in favorable cases, but this cannot be expected in
most instances—it is usually six months to a year. An opinion as to
the time required in a given case should always be guarded. A good
deal depends upon the patient’s care and perseverance in carrying out
the treatment. The disease often shows a tendency to recurrence.
The hair should not be allowed to grow for months after apparent cure,
shaving being persistently practised, experience teaching that this tends
to prevent relapses.
Ulerythema sycosiforme is extremely rebellious—much more so
than the ordinary sycosis.
Treatment.—The plan of treatment in most instances consists
of external means alone. The state of the general health should, how
ever, be inquired into, and proper treatment instituted to bring it up
to a normal standard. In some cases there is an underlying constitu
tional debility, which, unless corrected, seems to add to the obstinacy
of the disease; in such cases cod-liver oil is an admirable remedy, the
administration of which not infrequently quite perceptibly aids in ob-
SYCOSIS VULGARIS 1019
taining a result from local measures. Such tonics as iron, quinin, and
manganese will at times also apparently have a favorable influence.
Arsenic may be given for its tonic effect, but it has no specific action.
A special value has been claimed for calx sulphurata, given in doses of
from 1/10 to 1/4 grain (0.0065-0.016) three or four times daily, but my
experience with this drug has not been at all favorable. Sodium sal-
icylate in underlying rheumatic state and stomachic and digestive tonics
in dyspeptic cases will be of service. Alcoholic drinks, indigestible foods,
tobacco, excessive coffee or tea-drinking, and indulging in the many
“bromo” compounds now so common—all have a damaging tendency.
The bowels should always be kept free. Nasal catarrh, if present,
should receive attention. The influence of hygienic living and open-air
life and exercise is, without doubt, of value from a therapeutic stand
point. In obstinate and extensive cases, especially where the suppura-
tive factor is pronounced staphylococcic vaccine should be tried—as a
rule, the results are disappointing, but exceptionally its action is of con
siderable help.
In the external treatment the first steps are to clip the hair short,
free the parts from crusting, if present, and reduce the inflammatory
action. If necessary, the crusts can be removed with starch poultices,
but, as a rule, frequent bathing with warm water and soap and the appli
cation of plain petrolatum or cold cream will accomplish this end in a
day or two. Then mild soothing applications are to be made for a few
days until the activity of the inflammatory process is somewhat allayed.
This may be accomplished by means of applications of an ointment of
zinc oxid, of salicylated paste, or, in fact, by means of any of the other
mild ointments or lotions mentioned in the treatment of acute eczema.
As soon as the inflammatory action has been lessened, and, in fact, in
almost all cases from the very beginning, shaving every day or every
second day should be insisted upon as an essential part of the treatment.
This will not be without pain at first, which is by no means unbearable,
but after the first two or three shavings the operation is not especially
painful. It materially aids in rendering the treatment effective and in
shortening the time required for a cure, and this the patient soon recog
nizes himself. I value this so highly that I should decline to treat a
case unless this measure were acceded to. When the follicular inflamma
tion is of a markedly pustular character, and especially if the hair shows
a tendency to loosen, depilation may be practised; this tends to prevent
the permanent destruction of the follicles. As a routine procedure for
the whole diseased area, however, depilation is, in my experience, too
painful a practice to take the place of shaving, and I do not believe of
greater therapeutic value.
In the management of the external treatment of sycosis it is to be
kept in mind that as patients are often obliged to keep to their business,
the applications for the day-time should be scanty in quantity, or such
as do not conspicuously disfigure. The essential part of the treatment
consists in application of antiseptic ointments and lotions. In recent
and slight cases the applications to be described will usually be effective;
in extensive, long-continued, and obstinate cases these are also to be used,
1020
DISEASES OF THE APPENDAGES
but may be supplemented by the Röntgen-ray treatment. The former
will be referred to first. Ordinarily, the plan of making a slight applica
tion in the morning and applying the ointment spread upon linen or lint
as a plaster at night may be adopted; in the milder case the night appli
cations may also consist of simple anointing. In mild and sluggish types
the ointment, more especially at night, is to be gently, but firmly, rubbed
in. When lotions and ointments are used conjointly, the wash is first
dabbed on for a few minutes, allowed to dry, and then the salve is applied.
The parts should be washed once daily with soap and warm or hot water,
in irritable cases using a mild toilet-soap, and in sluggish and obstinate
types occasionally using sapo viridis or the tincture of sapo viridis. There
is no set guide as to the choice of a remedy among those commonly em
ployed; as a rule, in markedly inflammatory cases the use of a saturated
boric acid solution or a mild resorcin lotion, 0.2 to 1 per cent, strength,
followed by a soothing ointment, such as the boric acid ointment or dia
chylon ointment, will be most likely to be well borne. Later other
remedies will usually be demanded. Often enough one remedy will fail
absolutely to influence the disease favorably, or it may benefit for the
first week or two, and then cease to have any favorable effect; in either
event the remedy is then to be set aside and another tried; later a change
back to an application which had previously benefited can sometimes
advantageously be made.
Although occasionally one of the stronger remedies, such as a strong
sulphur ointment, can be used at the start, it is advisable, except in the
very sluggish cases, to begin with mild treatment, such as just mentioned.
A very weak sulphur ointment, 2 to 5 per cent., is, however, a safe begin
ning application. Or mercury oleate can be used, and is often of decided
benefit, prescribed as an ointment of from 20 grains to 1 or 2 drams
(1.3-8.) to the ounce (32.) of ointment base, of equal parts of cold cream
and simple cerate, or, if the quantity of the oleate is large, with all cerate.
Resorcin is commonly used as a lotion conjointly with a mild salve, as
already mentioned, although it may likewise be employed in the form
of an ointment. The strength of the lotion in chronic and sluggish cases
should be from 1 to 10 per cent.; of the ointment, from 5 to 10 per cent.
One of the most valuable external remedies is precipitated sulphur,
employed as an ointment in the strength of from 20 grains to 2 drams
(1.3-8.) to the ounce (32.) of petrolatum or cold cream; in the form of a
lotion, the Vleminckx’s solution applied diluted with from 5 to 15 parts
of water and supplemented with a mild sulphur or a boric acid salve or
cold cream deserves mention. Owing to its odor, this lotion is not a
pleasant remedy, and should be used only when other treatment has
proved unsuccessful. Hays has also found it of service. A compound
ointment as follows has been especially useful in some cases:
R. Sulphuris præcipitati, 3j (4.);
Balsami Peruvianæ, 3j (4,);
Unguenti diachyli, 3vj (24.).
It should be made up fresh every week or so, as the color becomes grad
ually darker and the ointment less efficient from chemical change.
SEBORRHEA
I02I
Ichthyol is another valuable remedy in the treatment of sycosis,
employed usually as an ointment in the strength of from \ dram to 2
drams (2.-8.) to the ounce (32.) of petrolatum, cold cream, or simple
cerate. In weakest proportion it is also a safe application for the begin
ning treatment. It may also, conjointly with an ointment, be employed
as an aqueous solution in from 2 to 10 per cent, strength. It may like
wise be used in an ointment of sulphur, with advantage, as follows: R.
Sulphuris præcipitati, 3ss-iss (2.-6.); ichthyol, 3j-iss (4.-6.); petrolati,
q. s. ad 3j (32.). Ehrmann warmly advocates the treatment of this
disease with a 10 per cent, solution of pyoktanin, introduced into the
diseased follicles by cataphoresis—the positive electrode, soaked in this
solution, is applied to the part, and the cathode held in the hand.
The Röntgen-ray treatment is occasionally found a valuable addi
tion to our means of treating this disease, and should be tried in per
sistent, extensive, and obstinate cases. The parts other than those to
be treated should be properly protected with lead foil. It need not be
added that the use of so potent an agent as the x-ray requires caution.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |