| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
CLASS VIII—DISEASES OF THE APPENDAGES
In the class of diseases of the appendages of the skin it is convenient
and customary to include not only affections of the appendages proper,—
the hair and nails,—but also those of the glandular structures as well.
They can be considered under four heads: 1. Diseases of the nails. 2.
Diseases of the hair and hair-follicles. 3. Diseases of the sebaceous
glands. 4. Diseases of the sweat-glands.
1. DISEASES OF THE NAILS
ONYCHAUXIS1
Synonym.—Hypertrophy of the nail.
Definition.—An overgrowth of the nail in any direction.
Symptoms.-—The affection may be congenital or acquired,
usually the latter. One or all of the nails may share in the process,
and the hypertrophy may take place in one or all directions, and this
increase may be, and often is, accompanied by changes in shape, color,
and direction of growth. It is not uncommon, too, to find conjointly
atrophic changes in some nails or parts of one or more nails, along with
the hypertrophic growth. Supernumerary nails, though scarcely to be
considered an example of hypertrophy, are occasionally noted. In ex
ceptional instances nail-formation has taken place on the stump ends of
amputated fingers, etc
Congenital hypertrophic changes are rare. Nicolle and Halipré2
had under observation a patient with congenital hereditary malforma
tion of the nails, with an associated atrophic condition of the hair. All
the nails of both hands and feet were involved and presented hypertrophic
growth, friability, and tendency to split and crack, and in some atrophic
changes; there also existed disposition to paronychia. A diseased con
dition of the nails could be traced through six generations, involving 36
members out of 55. White3 reports a somewhat similar interesting series,
1 Literature of diseases of the nails: Heller, Die Krankheiten der Nägel, Berlin,
1900 (a most admirable monograph, with many illustrations and a complete bibliog
raphy); Shoemaker, Jour. Cutan. Dis., 1890, pp. 334, 388, 419, and 476 (with references
and abstracts of interesting cases); Hutchinson, Arch, of Surgery, 1891, p. 237; D. W.
Montgomery, “Diseases of the Nails,” Twentieth Century Practice, vol. v (Diseases of
the Skin); Schwimmer, “Nagelkrankheiten,” Eulenberg’s Real-Enclyclopädie, 1898,
vol. xvi, p. 371; Pollitzer (inflammatory affections), Zeisler (trophic affections), Grin-
don (parasitic diseases), and Hardaway (treatment), Jour. Cutan. Dis., 1901, pp. 503-
527; Leisseur, ibid., 1902, p. 502; C. J. White (clinical study of 485 cases), Boston
Med. and Surg. Jour., Nov. 13, 1902; Jackson, Jour. Cutan. Dis., April, 1905, p. 153;
Hyde, “The Egg-Shell Nail,” Jour. Cutan. Dis., 1906, p. 145 (illustrated).
2 Nicolle and Halipré, Annales, Aug.-Sept., 1895, pp. 675 and 804 (with illustration).
3 C. J. White, Jour. Cutan. Dis., 1896, p. 220 (with illustrations).
952
ONYCHAUXIS
953
presenting both hypertrophic and atrophic changes, with subungual in
flammation, and, in one nail, paronychial inflammation. In this in
stance, too, with an occasional break, four generations had been affected
—in some congenital absence or malformation, in others changes taking
place later. The thin, downy, sparse hair was also noted, as in Nicolle
and Halipré’s case. Eisenstaedt1 met with a somewhat similar series
of cases—five generations.2 A congenital case of upward projecting,
thickened, claw-like nails has been recorded by Sympson,3 in which, too,
there was an occasional disposition to soreness. In this instance there
was no hereditary tendency.
Acquired onychauxis is, in its milder phases, not uncommon; its
extreme type is somewhat rare. The overgrowth sometimes consists
of simple thickening, which may be quite marked, or there may be a
hypertrophic tendency toward lateral growth, which sometimes results
in producing a periungual inflammation—paronychia. This latter may
be slight and consists of trifling inflammatory redness, or there may be a
good deal of swelling and purulent discharge. Many cases, however,
are seen in which no tendency to underlying or surrounding inflammation
is observed. In occasional instances the nail thickens enormously and
becomes relatively compressed laterally, so that it consists of a thick,
horny growth, somewhat flattened basal part, and more or less rounded
on the upper side, and either projects upward toward the distal end,
downward like talons (claw-nails), or may be slightly or markedly twisted,
like a horn—onychogryphosis. The large toe-nail is one especially liable
to malformed overgrowth. It is also seen on the fingers, and may in
volve one, several, or more nails; a typical example of the latter has been
reported by Ricketts4 In some cases the hypertrophied nail is hard
and horny, in others more or less friable and easily breakable in part or
throughout. The luster is usually lost, the nail-substance becomes
opaque, the surface often rough and irregular, and the color a dirty yel
low, brown, or even blackish.
Unna5 describes a persistent condition of the nails which I have
occasionally seen, and which he terms “scleronychia,” characterized by
thickening, inelasticity, hardness, roughness, and by being opaque and
of a yellowish-gray color, with disappearance of the lunula; there often
appear longitudinal furrows, or the surface may be made up of protuber
ances and depressions; the anterior border is rough and irregular, but
there is no tendency to chipping or breaking; it usually involves all the
finger-nails simultaneously, and sometimes the toe-nails as well. Mod
erate degrees of onychauxis are not uncommon in tuberculosis, the nails
being slightly or moderately thickened, broadened, with a tendency to
curve over the finger-ends. Invasion of the nails by the vegetable fungi
(onychomycosis) of ringworm and favus bring about, in some instances,
increase in size, along with the granular and friable condition noted.
1 Eisenstaedt, Jour. Amer. Med. Assoc, Jan. 4, 1913, p. 27 (with illustrations).
2 An interesting fact concerning these three series (Nicolle and Halipré, C. J.
White, Eisenstaedt) of cases is that the subjects were French or of French extraction.
3 Sympson, Lancet, 1888, i, p. 772 (with illustrations).
4 Ricketts, Cincinnati Lancet-Clinic, 1887, i, p. 302.
5 Unna, Histopathology, p. 1051.
954
DISEASES OF THE APPENDAGES
The various inflammatory diseases, such as psoriasis, eczema, etc, in
volving the finger and nail regions, are often responsible for a slight degree
of onychauxis. Very often, however, a thickening of the nail is more
apparent than real, the seeming increase in thickness being due to under
lying accumulation of epithelium or scaliness. A condition of this kind,
independent of any cutaneous inflammatory disease, and involving most
of the finger-nails, was observed by Hallopeau and Le Damany,1 who
designated it as a generalized parakeratosis of the nails, the thickness
being due to imperfect keratinization of the lower layer. Sometimes the
nails, especially in their distal half, are decidedly raised from the nail-bed
by a growth of horny material beneath them.2
In onychauxis knocks and even the free use of the parts sometimes
lead, owing to the unyielding characters of such nails, to tenderness
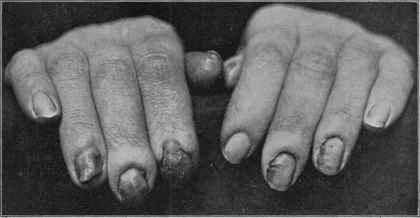
Fig. 239.—A chronic condition of onychia and paronychia with atrophic (and some
times associated hypertrophic) nail changes, slight bulbous swelling of the finger-ends;
occasionally seen as an idiopathic affection, but more usually associated with eczema of
the fingers, and occurring most commonly in women, and more particularly in those
who have their hands in water a great deal. Occasionally this condition is seen in asso
ciation with or following impetigo contagiosa, or independently as a staphylococcic
infection of the nail-beds and nails; sometimes doubtless of streptococcic origin.3 It
may be occasionally accompanied with arthritis of the distal joints.4
or a variable degree of inflammation of the nail-bed (onychia) and the
surrounding tissue (paronychia, whitlow). Onychia may exist, however,
primarily and lead to atrophic or hypertrophic nail change; the matrix
is often considerably inflamed, and is sometimes accompanied with a
seropurulent undermining, but more frequently the nail-bed and peri-
ungual tissue both share in the inflammatory action. The onychial in-
1 Hallopeau and Le Damany, Annales, 1895, p. 538.
2 Malcolm Morris, Brit. Jour. Derm., 1901, p. 8, exhibited a striking case of this
kind, a boy of twelve, and A. G. Wilson, ibid., Jan., 1905, p. 13 (with illustrations and
references), has reported cases of similar character as a hereditary affection—three gen
erations.
3 Adamson, Brit. Jour. Derm., 1904, p. 165, describes a case following impetigo,
with references.
4 Hartzell, “Diseases of the Nails, Accompanied by Arthritis of the Distal Joints of
the Fingers and Toes,” Univ. Med. Bull., Oct., 1904 (with two illustrations).
ONYCHAUXIS
955
flammation may be of a malignant character, with destruction of tissue
and involvement of the lymphatics; the nail is cast off, and discloses a
markedly inflamed, suppurative tissue. The affection rarely involves
more than one or two nails.
Simple paronychia is often independent of hypertrophic nail changes,
and is commonly seen about a toe-nail, being simply the result of lateral
pressure of a normal nail produced by tight-fitting shoes, or from a slight
overgrowth laterally (ingrowing nail). It is likewise observed, however,
about the finger-nails, and here the paronychial inflammation may be
extremely sluggish, quite superficial, consisting of redness and slight,
sometimes scarcely perceptible, swelling, and with little, if any, tendency
to purulent formation or accumulation; in such cases several or more of
the fingers are involved, and this type of the affection is usually observed
in those who are obliged to have their hands in water a great deal. A
mild degree of onychia may be present. It is also observed in association
with eczema of the fingers. In other instances the inflammatory action
is more intense, with considerable pain, swelling, and pus-accumulation.
The nutrition of the nail often suffers.
Both in onychia, and paronychia the involved area may exception
ally be small, consisting of only a part of the nail region, usually forward
and laterally, and may so persist, unless treated, indefinitely, sometimes
gradually, but scarcely perceptibly, from day to day, extending.
Etiology and Pathology.—The etiology of onychauxis has
been already incidentally touched upon. The condition is more com
mon in advancing years. Pressure and warmth, doubtless, are of eti-
ologic importance in hypertrophy of the toe-nails. Lack of proper care
is probably contributory. The various chronic inflammatory cutaneous
diseases are sometimes responsible both for hypertrophic and atrophic
changes.1 Local irritation or injuries, constitutional disorders, gout,
rheumatism, and diseases of the nervous system, or injuries involving
the nerves, as in Bowlby’s case,2 may also be, to a varying degree, pro
vocative of hypertrophy. Thickened and enlarged nails are sometimes
seen in acromegaly, and may also be observed in some cases of leprosy,
syringomyelia, and similar affections, although atrophic conditions are
probably more common. An explanation of why, in some cases, the
overgrowth should take one direction, in other cases another, and in still
others a twisted, hornlike form and character is difficult to find; pressure
is, it is true, a directing influence in some instances, but not in all.
Onychia is probably often idiopathic, due to slight traumatism or
1 C. J. White, loc. cit., found 404 out of 485 cases to be due to or associated with
6 diseases: eczema (107), trauma or felon (72), paronychia (68), psoriasis (67), occupa
tion dermatitis (62), and syphilis (28). Among comparatively new occupations which
may have a damaging influence on the nails, as well as the skin, may be mentioned that
having to do with the handling of formalin. Galewsky (Münch, med. Wochenschr., Jan.
24, 1905, vol. lii, No. 4, calls particular attention to the seeffects, which sometimes, as
regards the nails, may not follow till weeks or a few months after exposure. The condi
tion is often accompanied with a burning or boring sensation in the ends of the fingers
and the nails. A few instances of such occurrence among surgeons and nurses have
come under my own observation.
2 Bowlby, “Some Trophic Lesions Following Injuries of Nerves,'’ Illustrated News,
1889, vol. iv, p. 25 (with colored plate showing marked hypertrophy and transverse
furrows).
956 DISEASES OF THE APPENDAGES
persistent or repeated irritation from a hypertrophied nail, which serves
to give chance to a localized pyogenic infection. Syphilis and tubercu
losis are also factors in some cases. The essential causes in paronychia
are pressure, and possibly a variable but mild local pyogenic infection.
Unskilled manicuring and infected manicuring instruments may also
play a part.
Treatment.—The result of treatment, especially as to perma
nency, in these various conditions will depend upon a proper recognition
of the essential causative element. A coexisting disease, cutaneous or
systemic, will often be the clue which indicates the line of constitutional
treatment. Cod-liver oil, tonics, and mercurials, with potassium iodid,
may, therefore, be variously needed. Arsenic is valuable in some cases,
but it must be persisted in to get a result. Unna found it curative,
though slowly, in scleronychia. In some cases the cause is found to be
purely an external one, and the treatment, therefore, wholly local. In
others, again, the disease seems idiopathic, so far as our knowledge goes,
and exists without any demonstrable reason, and in such cases the man
agement is purely empirical, usually local and general. For ordinary
onychauxis of one or two nails, local measures alone are called for.
Proper care and cutting of the nails, the avoidance of pressure, either
from tight-fitting shoes or gloves, are essential. Even slight injuries or
traumatisms with manicuring implements should be guarded against. The
excessive nail-growth should first be thoroughly softened by soaking in
hot water, in which a little sodium bicarbonate or borax has been dis
solved, and then carefully cut or filed away. Subsequent overgrowth
can usually be kept under control by a fine file rather than with the scis
sors or knife. If there is a tendency to stony hardness and brittleness,
a slight soaking nightly, or every second or third night, in hot water,
with or without the addition of the alkali, is advisable, the part being
subsequently enveloped over night with a plain ointment, such as cold
cream or vaselin.
Onychia, if of mild character, can sometimes be managed by frequent
washings of the parts with saturated solution of boric acid and continuous
applications of a 25 to 50 per cent, ointment of ichthyol. Salicylic acid
ointment, with equal parts of lanolin and cold cream, 3 to 10 per cent,
strength, is also valuable. If the nail is hard and inelastic, occasional
softening by soaking in a warm solution of sodium bicarbonate, 4 or 5
grains to the ounce, is advisable. Occasionally painting thoroughly
both around and under the edges of the nail with a 2 to 5 per cent, solu
tion of silver nitrate in sweet spirits of niter proves serviceable; if done
carefully, the solution can be well insinuated (“flowed in”) under the
ends and sides of the nails, and thus come in contact with a great part of
the diseased area. Not infrequently, however, removal of the nail
may be necessary. If there is undermining suppuration, incisions are
advisable, the subsequent applications being the same as above. In
these latter cases, instead of ichthyol ointment, after washing with the
boric acid solution the part can be enveloped in a thick layer of boric
acid powder. The dressings should be changed two or three times daily.
In obstinate cases, especially those of distinctly suppurative or pyogenic
ATROPHIA UNGUIUM
957
type, both as to onychia and paronychia, x-ray treatment can some
times be used to advantage.
Paronychia is to be managed in the same manner as onychia as re
gards the applications. Unhealthy granulations, if present, can be
modified or destroyed by applications of silver nitrate—stick or solu
tion. If due to apparent side pressure of the nail, the center of the nail
should be filed somewhat thin, and a small tuft of cotton or lint, wet with
boric acid solution, gently insinuated under the lateral nail-edges to re
move the pressure. Occasional softening with bicarbonate of sodium
solution is also of value. In most cases, those of mild character, these
measures will, if faithfully carried out, usually suffice. If there is con
siderable lateral pressure, due to nail overgrowth, the side edges can be
carefully trimmed off; or if the case is a severe one, avulsion of the nail
may be necessary. In operations about the nails complete or relative
anesthesia can be produced by cocain. In the milder types, those of
sluggish and persistent character, observed about the finger-nails, the
several applications referred to, along with general tonic treatment when
needed, and keeping the hands out of water, will often bring the affair
to an end. Arsenic is useful in some of these cases. Cooks, laundresses,
etc, continuously obliged to have their fingers wet a considerable part
of the time, should have recourse to rubber gloves while at such work.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |