| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
ACNE
Synonyms.—Acne vulgaris; Acne disseminata; Acne simplex; Fr., Acné; Ger.,
Acne vulgaris; Akne; Finnen.
Definition.—An inflammatory disease, usually chronic, of the
sebaceous glands of the face, face and shoulders, upper trunk, and occa
sionally of the back, characterized by papules, tubercles, or pustules,
and sometimes nodules, or a combination of these lesions, and commonly
met with between the ages of thirteen and thirty.
Symptoms.—The most common site for the disease is the face,
and it is generally limited to this region; in many cases, however, it
is not infrequent to see several lesions, and sometimes a large number,
on the neck and shoulders as well, and occasionally some on the upper
trunk; exceptionally the back is the chief seat, extending from the neck
to the sacrum, and in rare instances the eruption may be limited to this
latter region, with lesions also on the anterior surface of the trunk.
The eruption may be insignificant, consisting of but several or
more scattered lesions, or it may be abundant; in average cases there
are usually 30 to 40 present. Exceptionally the eruption may appear
somewhat acutely, a moderate or large number of lesions presenting in
the course of one or two weeks; as a rule, however, it begins slowly and
insidiously. The eruption is generally made up of small pale-red, bright
1 Van Harlingen, Handbook of Skin Diseases.
ACNE
1037
or dark-red pin-head to pea-sized or larger papules and some pustules.
The base is slightly, moderately, or markedly inflammatory. Taking
a common example of the disease, there will be noted, irregularly scattered
over the face, usually more numerous on the forehead, chin, and over the
lower jaw, 30 to 50 pin-head to pea-sized papules, tubercles, or pustules,
or, more frequently, a mixture of these lesions (acne vulgaris), and in the
various stages of evolution and involution or subsidence; interspersed
are usually to be seen comedones (blackheads), and not infrequently the
same formation or the blocked-up gland-duct is readily recognizable
in the center of the apex of the smaller papules. The lesions may be
somewhat acute in character, with a hyperemic inflammatory base,
or they may be sluggish; or some are distinctly inflammatory and
others but sluggishly so.
In many of these cases the
skin seems relaxed, thick,
dirty, and greasy, usually
from a slight or moderate
oily seborrhea which fre
quently coexists; in such
instances particularly the
gland outlets are often large
and quite conspicuous. If
a pustular lesion is squeezed,
a mixture of pus and seba
ceous matter is discharged,
and occasionally a small
thickened mass which
faintly suggests a core. In
the course of several days
or a few weeks pustular
lesions have dried or been
broken and discharged and
partly or completely dis
appeared; papules, and
tubercles if present, will
have gradually vanished by
absorption, or, as more
commonly occurs, they be
come pustular, and rapidly
or slowly dry or discharge, and disappear, usually without leaving a
trace more than a reddish stain, which finally fades. During this time,
however, new lesions are presenting and going through the same evolu
tion and involution stages. Thus the case goes on, with slight or marked
fluctuations between better and worse—slight and relatively few in num
ber at times, sluggish or inflammatory and the lesions numerous at other
periods. In many cases, after some months to several years, or more,
the eruption may, and frequently does, begin to decline, the new lesions
gradually diminishing in numbers, and finally the patient is entirely free.
In other instances there may, on the average, be but 5 to 10 lesions

Fig. 258.—Acne of small papular and papulo-
pustular type, with numerous comedones—“black-
heads.”
1038 DISEASES OF THE APPENDAGES
present, and with intervals of several days or a few weeks in which no
eruption at all is to be seen; several cropping out irregularly when the
patient suffers from digestive disturbance, constipation, and in girls and
women at the menstrual epochs. On the other hand, in some patients
100 or 200 or more are found, here and there close together or irregularly
scattered, not only over the face, but the shoulders and upper part of the
trunk. In occasional cases the hyperemic element is quite pronounced,
and if the lesions are near together, the condition and appearances ap
proach those of acne rosacea.
The above is the usual picture encountered, and generally no scarring,
or no perceptible scarring, results, the patient finally recovering without
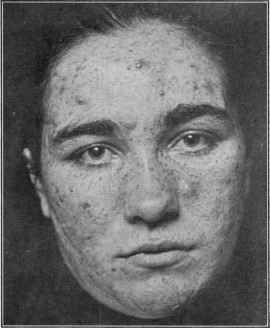
Fig. 259.—Acne of the papular, pustular, and indurated or boil-like type, with
a general “muddy” complexion, in a woman aged twenty-two, of several years’ dura
tion; some minute, pit-like scars left by former lesions are noticeable on the cheeks.
a trace of the previous eruption. This is, however, unfortunately not
always so, as slight tissue destruction or atrophic changes producing per
manent marks sometimes occur, and in such cases this tendency dis
tinctly predominates so that the marks are usually quite numerous.
The large, purulent, deep-seated lesions and the dermic abscess type to
be referred to often leave very distinct cicatrices.
The so-called clinical varieties are named from the predominant
type of lesions present, and from the accidental or coincident character
of the inflammatory process and the resulting changes. Thus an acne
lesion usually begins by a blocking-up (comedo) of the sebaceous gland
outlet and a mild degree of hyperemia and inflammation results, which
ACNE
l039
causes a slight elevation, generally with a central blackish or dirty gray
or yellowish point, and the majority or most of the lesions may exhibit
but little tendency to advance beyond this stage, and such instances
constitute acne punctata. As a rule, however, the inflammation is of
higher grade or the lesion progresses, producing a more prominent,
usually small pea-sized, reddish, papular elevation, probably due to peri-
follicular infiltration, with but little tendency, in most of the papules,
to advance to suppuration, and thus is presented acne papulosa. If
the inflammatory action is still more intense, or continues, or probably
if micro-organisms invade the lesions, they or the most of them tend to
advance rapidly to central suppuration, especially toward the apex.
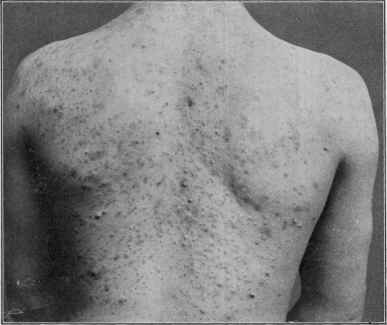
Fig. 260.—Acne of the back—showing pustules, papules, and blackheads; the scar
ring which is often quite marked in back cases is not conspicuous in this instance
(courtesy of Dr. M. B. Hartzell).
and pea-sized or larger formations present, which show, under the thinned
epidermal covering, pustulation; such cases represent the so-called acne
pustulosa. In some patients the inflammation begins somewhat deeply,
and is felt as subcutaneous nodules, which grow larger and toward the
surface, and then remain as small or large pus cavities, very slowly under
going resolution, or finally break and discharge, and then may again
fill up; others show pustulation, and at the same time the base becoming
markedly inflammatory and hard—acne indurata. In some instances,
fortunately not common, of the smaller lesion cases, usually small papu
lar, or less frequently pustular, as the lesions disappear they leave a
pit-like atrophy or depression—distinct though not large scars—and
1040 DISEASES OF THE APPENDAGES
this represents the type known as acne atrophica. When such tendency
does exist, it is exhibited by most of the lesions. On the other hand, in
some such cases slight connective-tissue new growth may follow their
disappearance and present as minute or small scar-tissue or keloidal
elevations—acne hypertrophica. In other instances, not very numerous,
and usually observed in those of cachectic and depraved condition, the
gland itself seems to be the seat of the chief inflammatory and suppurative
changes, and furuncular or sluggish abscess-like formations result, which
may show but little, or an extremely slow, tendency to break through;
many of these lesions are of the nature of dermic abscesses, usually of a
cold, sluggish character, and sometimes of more general distribution—

Fig. 261.—Acne of back—somewhat large papulopustular and nodular type, with some
scarring.
acne cachecticorum. Under this latter name, but preferably under the
designation of acne scrofulosorum, is also to be included a sluggish papular
or papulopustular acne of livid red color, pea- to cherry-sized, observed
associated with strumous symptoms, and commonly occupying the
trunk and extremities, and less frequently the face also; slow in evolution,
and sometimes slight superficial destruction occurring under the crust
and leaving scars.
Acne cases are occasionally encountered in which the eruption is
almost entirely or wholly limited to the trunk, usually or more par
ticularly the back and the breast, and in such instances the eruption,
as a rule, consists of numerous variously sized papular, papulopustular,
ACNE
1041
more or less indurated sluggish lesions, with, in some, a tendency to the
dermic abscess type; many comedones, some double and multiple, are
also generally present. The eruption is sluggish and persistent, old
lesions going slowly and new presenting; considerable scarring is some
times noted.
The lesions in acne are discrete and scattered, but occasionally a
tendency is exhibited here and there toward the formation of several
somewhat closely set groups; in such the base seems almost continuous,
as in some of the iodid and bromid eruptions. In the dermic abscess
variety this tendency to contiguous formation is also now and then
observed. While most lesions probably have their beginning in a block-
ing-up of the gland outlet, this is not demonstrable in all, and more es
pecially not in the deep-seated formations.
Acne artificialis is a term applied to the acne-like eruption pro
duced by the ingestion of the iodin and bromin preparations, also named
iodid or iodin acne and bromid or bromin acne; and from the external
use of tar (acne picea, acne picealis) in occasional instances. This
latter is likewise met with in those who, in the course of their work, are
brought into frequent contact or live in an atmosphere strongly impreg
nated with tar or tarry products. Tar acne results from a blocking-up
of the follicular openings with this product. With tar acne furuncles
are often associated. Chrysarobin is noted at times to bring about
follicular inflammation and acne-like lesions. Workers in petroleum
and paraffin products are also occasionally the subjects of acneiform,
furuncular, and abscess formations. These several artificial eruptions,
which may be limited or more or less general, are referred to under the
head of Dermatitis medicamentosa or Dermatitis venenata.
Another variety or acne-like eruption, often limited to the face,
as in 2 of my cases, sometimes seen on the face, scalp, neck, and shoulders
also, and in others upon the extremities as well, and deserving of the name
of acne urticata (Kaposi, Touton, Löwenbach, and others) ,1 already given
to it, is that in which the lesions suggest both acne and urticaria. Pre
ceded, as a rule, by itching, they begin as small or ordinary sized pinkish
or reddish, urticaria-like elevations or distinct wheal-like lesions, which
enlarge somewhat and soon exhibit slight central vesiculation, which
dries to a thin crust, during which time the urticaria-like basis usually
has entirely disappeared. Beneath the crust some necrotic or atrophic
action takes place, and when it drops off, a small depressed scar remains.
If the formation is squeezed before crusting and desiccation ensue,
there appears a small amount of serum, but no pus. The course of a
lesion is generally run in from one to two weeks, but new eruption con
tinues to appear and the disease lasts indefinitely. It is not a frequent
variety, nor is it, I believe, a true acne, but probably a type (Kaposi) of
acne varioliformis; its clinical symptoms and behavior are somewhat
similar. Löwenbach’s investigations give it a middle position between
1 Kaposi, Pathologie und Therapie der Hautkrankheilen, 4. Auflage, Wien, 1893,
p. 529; Touton, Verhandlungen der Deutschen Dermatologischen Gesellschaft, VI. Con
gress, 1899, p. 7 (this paper covers all varieties and types of disease described under the
name acne, with full bibliography); Löwenbach, Archiv, 1899, vol. xlix, p. 29 (with
histologic study, reference to allied diseases, and bibliography of same).
66
1042
DISEASES OF THE APPENDAGES
acne varioliformis and urticaria perstans. The several cases under my
care were all neurasthenic girls between eighteen and twenty-five, and
of weak digestion. The cause is not known; micro-organisms have been
found, but with no uniformity. In all my cases and those of others
(Kaposi, Touton) digestive disturbances were noted. Its anatomic
seat is about the hair-follicle. The disease is stubborn and rebellious
to treatment.
Under the name of acne keratosa1 Crocker has described 4 cases
of a rare affection, one of which had been previously recorded by Jamie-
son, possessing some of the features of acne. The eruption is seen on
the face, on the chin and cheeks, and commonly near the corners of the
mouth. Red, tender, firm lumps, persistent in character, are first seen,
on which pustulation usually presents, and dries to a crust. Sometimes
the covering epidermis is detached by the underlying lymph. On re
moval of the crust, one or several soft or horny conic “pegs,'’ about
1/12 inch long, which produce irritation, are found embedded; their re
moval is followed by gradual but very slow disappearance of the lesion,
usually leaving scars. New formations appear from time to time, and
the disease goes on almost indefinitely. In some cases there is an irre
sistible desire for the patient to pick at them, resulting in excoriations,
as in Brocq’s2 patients. The lesions have their seat in the sebaceous gland
or hair-follicle. The cause of the disease is unknown, and treatment,
similar to that of ordinary acne, not very satisfactory.
The course of acne is almost always persistent, individual lesions
disappearing after a variable time—several days to several weeks,
according to character, but new lesions making their appearance irreg
ularly from day to day or week to week. In average examples scarring
does not result. As already remarked, cases vary much in the number,
features, and behavior of lesions. Some are so slight, the lesions so few,
and the parts often free, that they scarcely are entitled to be considered
a disease; on the other hand, many are troublesome and disfiguring to
a repulsive degree. As the patient advances toward full growth and
enters adult age in many instances the tendency disappears, but this is
by no means true in all.
Ordinarily there are no subjective symptoms in average acne cases,
occasionally slight beginning soreness, and when the inflammation is
marked there may be tenderness, especially upon pressure. Excep
tionally there is moderate itching, particularly just as the lesion is about
to appear.
Etiology.3—The disease is a frequent one. The causes are
1 Crocker, “Acne Keratosa,” Brit. Jour. Derm., 1899, vol. xi, p. 1; Jamieson,
“Peculiar Ulcerative Eruption of the Face, Associated with the Formation of Horny
Plugs, Accompanied with Pain and Apparently Developing in the Sebaceous Glands,”
ibid., 1893, vol. v, p. 141.
2 Brocq reported, under the name “L’acné excoriée de jeunes filies,” Paris, 1898, a
somewhat similar condition, in which, however, there were no horny pegs.
3 Bearing upon some etiologic factors named and treatment: Lomry, “Untersuchun-
gen über die Aetiologie der Acne” (bacteriologic), Dermatology Zeitschr., Aug., 1896—full
abstract in Brit. Jour. Derm., 1896, vol. viii, p. 453; Hodara, “Ueber die bacteriologische
Diagnose der Acne,” Monatshefte, 1894, vol. xviii, p. 573; Jacques, “De l’état sebor-
rheique de la peau et des ses rapports avec les dermatoses, notamment avec l’acné;
ACNE
I043
varied. The pus organisms are credited with being etiologic, but recent
investigations (Unna, Gilchrist, Hodara, Sabouraud, Beck, Fleming,
Engman, and others) point rather to a special bacillus—acne bacillus.
Sabouraud believes the bacillus brings about the seborrhœa often
noticed, and to this is added a special coccus (Staphylococcus albus
butyricus) for the acne. The evidence so far seems to indicate that the
bacillus and Staphylococcus albus are both factors, the former more or
less specific in most cases, the latter specific in some cases, but usually
contributory.
Admitting a parasitic agent, which now seems fairly well assured,
there are to be considered the predisposing causes which bring about
the proper condition of the skin (proper soil) for parasitic invasion or
prejudicial action,1 and without which predisposing or contributory
causes the parasitic agents may, in many persons at least, be found in the
skin without becoming pathogenic. These seem, indeed, in certain
cases distinctly etiologic; such are digestive disturbances (producing
reflex hyperemia of the parts (Crocker)), constipation, menstrual irregu
larities, chlorosis, general debility, lack of tone in the muscular fibers
of the skin, and scrofulosis. And as external factors may be mentioned
working in a dusty or dirty atmosphere, lack of cleanliness, the infre
quent use or entire abstention from the use of soap for the face. In fact,
anything which tends to block up the gland outlet has an etiologic bear
ing. Drug and trade factors have already been referred to—bromin
and iodin preparations, tar, and petroleum products. Indulgence in
the so-called “bromo” proprietary headache medicines is not an infre-
étude de pathogénie et de traitement,” These de Paris, 1892—abs. in Annales, 1892,
p. 1047; Mitour, “Etude sur la nature et le traitement de la dyspepsie accompagnée
acne,” These de Paris, Jan., 1896; Sabouraud, “La seborrhœe grasse et le pelade,”
Annales de l' lnstitut Pasteur, .1897, p. 134; Schütz, “Klinisches über Akne und der
seborrhoischen Zustand, Archiv, 1895, vol. xxx, p. 203; S. Mackenzie, “Etiology and
Treatment of Acne” (with discussion thereon), Brit. Jour. Derm., 1894, vol. vi, p. 304;
Unna, Histopathology, 1896, pp. 357, 361; Gilchrist, Trans. Amer. Derm. Assoc. for
1899, p. 97; and Jour. Cutan. Dis., 1903, p. 107 (with histologic and bacteriologic
illustrations, review and bibliography as to these subjects); Fleming, “On the Etiology
of Acne Vulgaris and its Treatment with Vaccines,” Lancet, April 10, 1909, p. 1035;
and “Vaccine Treatment of Acne Vulgaris,” Brit. Jour. Derm., 1910, p. 6; Engman,
“Bacteriology in Certain Diseases of the Skin,” Jour. Cutan. Dis., 1910, p. 553; and
“Treatment of Acne Vulgaris with Acne Bacillus Suspensions,” Interstate Med. Jour.,
1910, xvii, No. 12; Gilchrist, “Vaccine Therapy as Applied to Skin Diseases,” Jour.
Cutan. Dis., 1910, p. 568; Towle and Lingenfelter, “Vaccine Therapy in the Treatment
of Diseases of the Skin at the Massachusetts Hospital,” Jour. Cutan. Dis., 1910, p.
583; Lasseur, “Le Traitement de l’acne pustuleuse par les Vaccines,” Annales, 1910,
p. 377; Lovejoy and Hastings, “Isolation and Growth of the Acne Bacillus,” Jour.
Cutan. Dis., 1911, p. 80; Morris and Dore, “Treatment of Acne by Vaccines,” Brit.
Jour. Derm., 1911, p. 3ii (review of organisms and therapy; regard vaccine treatment as
an adjuvant, occasionally brilliant, used both vaccines separately or mixed, choice
depending upon active organism; bibliography); Haase, Jour. Amer. Med. Assoc, Aug.
17,1912, p. 504 (gives a good review of the subject of bacterial findings, with references);
Lovejoy, “Treatment of Acne with Stock and Autogenous Acne Bacillus Vaccines,”
Amer. Jour. Med. Sci., 1912, p. 693.
Varney and Clark, Jour. Cutan. Dis., 1912, p. 72, found a micrococcus with unusual
characteristics as a factor in a resistant dermatitis resembling acne vulgaris—5 cases are
described; these were uninfluenced by the usual acne therapy, but were responsive to
the vaccines made from the organism.
1 Gilchrist believes that many of the constitutional and other symptoms often found
associated with the disease, instead of being predisposing causes, as commonly thought,
are, in fact, probably the result of absorption of the toxins of the bacillus acnes.
1044
DISEASES OF THE APPENDAGES
quent cause of scanty and irregularly appearing lesions. The not
uncommon custom of taking the advertised “blood-purifiers” in the
spring, most of which contain potassium iodid, is another element which
adds to dermatologic practice. In fact, I have met with several instances
in which the administration of the iodids or bromids was the starting
causative factor in the production of rather persistent acne. The use
of irritating soaps, but more especially soaps containing tar or its de
rivatives, is a contributing agent in some cases.
The most easily demonstrable contributory causes in many cases,
and which patients themselves soon recognize, are constipation and di
gestive disturbances. Night or day indulgence in indigestible foods,
in beer or other alcoholic drinks, will often provoke a fresh outcropping
in those with acne tendency. It is probably due to such causes that
acne of rather acute character, is occasionally met with in patients who
have just recovered from a severe illness—the appetite being keen, in
dulgence and overeating bring about indigestion or result in the absorp
tion of incompletely digested food. It is especially fermentative dys
pepsia (Hallopeau, Robin, Leredde, Elliot, Barthélemy, Jacques, Mitour,
and others) that is particularly etiologic; dilatation of the stomach
(Barthélemy)1 is also a frequent factor. Excessive tea- and coffee-
drinking and too free use of tobacco must also be considered to have
influence. Circulatory weakness, as evidenced by cold feet and hands,
is credited with influence, but this itself is doubtless often the result of
digestive difficulties. Menstrual irregularity or difficulty or other uterine
disorders is also a source of aggravation, if nothing more, in some cases,
and in those due to such cause a special tendency to appear on the chin
and around the mouth has been noted by some observers (Hallopeau
and Leredde). Women with acne are almost invariably worse at the
menstrual period, and mild cases will often be relatively or entirely free
in the interim. Another known fact is that the disease is commonly one
which belongs between the ages of thirteen and thirty; exceptionally it
begins earlier, and not infrequently it persists after the latter age, but
rarely presents for the first time after that period. It is common to both
sexes, among rich and poor, but it is somewhat more frequent in in
dividuals of light complexion, and in those leading a sedentary life.
Both excessive sexual indulgence and sexual continence have been as
cribed as factors, but with scant foundation.
Pathology.—Acne is pathologically an inflammation of the se
baceous glands, which may, from resulting suppurative action, mean
more or less follicular destruction. The attached lanugo hair-follicle
is usually implicated, and it is alleged by some writers that this is the
primary seat of the inflammatory action or irritation. In most lesions
an important step in originating the process is a blocking-up of the
glandular outlet, either by a comedo formation, as a result of a hyper-
keratosis (Unna), or from extraneous material; in the production of
1 Barthélemy, “Etiologie et Therapie de l’Acné,” Arch. gen. de méd., 1889, ii, p.
641; also in Monatshefte, 1889, vol. ix, p. 406. In 169 cases especially investigated
as to dilatation of stomach Barthélemy claims to have found this condition in 165—dys
pepsia in all, the first effect of improper digestion, according to this author, being a
seborrheic condition, and then the implantation of a pathogenic organism.
ACNE
1045
the former, atony of the muscular fibers of the skin, and especially
the arrectores pili,. is probably an important factor. Blocking-up of
the glandular outlet, however, is not sufficient explanation, for it is not
invariably observed, and it frequently occurs (see Comedo) without
any resulting irritation or acne lesion. To this, therefore, must be
added as yet an unknown agent, but which may variously be micro-
organisms, chemical and irritating change in the secretion within the
gland (Virchow), or some poison or irritant eliminated by the glands
(Leloir, Hallopeau, Leredde, and others), probably due to imperfect
digestion; the first named, in the light of our present knowledge of
cutaneous pathology, being most probable as the essential element.
The various conditions named in etiology prepare the soil for para
sitic invasion, seborrhea holding a prominent place. As also referred
to in etiology, ordinary pyogenic or similar organisms, which are some
times, but not always, present, have been thought to be the pathologic
exciting factor, but this has been called in question. More recently,
as already stated, a special bacillus, which Gilchrist finds has pus-pro-
ducing properties, has been found; it is somewhat short and thick, rod-
like, straight or curved, and sometimes branching, and occasionally
coccoid in form (Unna, Gilchrist). Gilchrist found this bacillus in every
acne pustule examined.
According to investigations (Simon, Virchow, Hebra and Kaposi,
Biesiadecki, Leloir and Vidal, Robinson, Elliot, Heitzmann, Gilchrist,
and others), the inflammation begins either in or around the gland,
the vessels showing engorgement; in the latter event the glandular
structure becomes secondarily involved. Inflammatory infiltration
may be somewhat limited, and chiefly around the gland-outlet, or be
periglandular, or it may be quite extensive and diffused, and even in
volve several glands. Suppuration generally ensues, but this is a
secondary result, and not necessarily constant. The infiltration,
which may be superficial or deep in the derma, is inflammatory in char
acter, with sometimes plasma, large fusiform, giant- and mast-cells,
and, when suppuration ensues, with leukocytes added. The epithelial
lining usually becomes thinned, extended, and may disappear entirely
when the glandular walls give way, the lesion being then a small, variably
sized, dermic abscess. Leloir and Vidal, who are among those who be
lieve the primary inflammatory changes to be perifollicular, have noted
in some instances suppurative foci around the glandular structure, which
eventually rupture into the cavity.
The contents are composed of seropurulent fluid, sebaceous matter,
and tissue débris. In the larger lesions not only the sebaceous gland
partly or completely suffers destruction, but the hair-follicles as well.
The character of the lesion is determined by the activity and intensity
of the process; inflammatory infiltration around the gland-outlet giving
rise to the smaller papules, and, when more extensive and periglandular as
well, to larger indurated papules and tubercles; and, when suppurative
action ensues, to the pustule. If the suppurative action is abundant,
the small dermic abscess results, and when intense, deep-seated, and
involving several glands, the large dermic abscesses are formed.
1046 DISEASES OF THE APPENDAGES
Diagnosis.—There is rarely any confusion possible in acne, if it
be remembered that the eruption is always folliciular and limited to
certain parts, and commonly the face alone, and that the several stages
of the lesions, from the blocked-up gland-outlet, or comedo, to the
papule and pustule, are usually present, not grouped, but discrete and
irregularly scattered. A history of some duration is ordinarily given.
While the lesions of pustular syphiloderm bear some resemblance, these
are almost always a part of a generalized eruption, with other symptoms
and a different course and history. The tubercular syphiloderm, and
also the tuberculopustular syphiloderm, usually late manifestations
and somewhat limited, if occurring on the face, are to be differentiated
more especially from large papular acne or acne indurata, but they are
differently colored,—copper or ham tint,—almost always grouped, and,
as a rule, in a circinate, segmental, or serpiginous manner; moreover,
they are slow in evolution, and frequently present underlying ulceration,
and leaving behind atrophy, staining, or scarring. The dermic abscess
variety of acne lesions is entirely different in its evolution, behavior,
and course from a gummatous syphiloderm.
An acute outbreak of acne has been mistaken for a beginning variola,
but if the distribution of the latter, its prodromal and accompanying
constitutional symptoms, are considered, such an error seems scarcely
possible. Acne is to be distinguished from acne rosacea by the facts
that the latter is more or less diffusely hyperemic, with, as a rule, dilated
vessels, and the eruption is usually predominantly about the nose and
immediate region; in extensive cases the region involved is an ovalish
area, of which the nose is the center, and the outer boundaries, the chin,
central forehead, and middle of the cheeks. Acne rosacea is, moreover,
much more common after the age of thirty, whereas ordinary acne then
becomes much less frequent. Midway types are, however, met with,
which partake really of the nature of both diseases.
Acne limited or more or less confined to the back differs from ordinary
cases simply in being in an unusual location, but its features are the same,
commonly of a more pronounced type than generally seen on the face;
there are frequently many comedones.
The possibility of acne-like pustules from bromin and iodin prepa
rations is not to be lost sight of; the lesions are usually a brighter red,
with, as a rule, a less pronounced base, and the contents are somewhat
thinner, and while lesions are almost invariably on the face, they are
often seen also on other parts on which acne is not observed; a safe plan,
however, in suspected cases is to make inquiry as to the ingestion of such
drugs.
Prognosis.—Acne is often a troublesome disease, sometimes
rebellious and obstinate; still, upon the whole, it is, I think, to be con
sidered one of the more favorable of the cutaneous maladies, and one in
which the results of well-directed treatment are usually gratifying.
The majority of cases respond quite readily, the skin clearing up in
the course of a few months; in others again somewhat rapidly at first,
and then more slowly, six months to a year or more being required to
bring about permanent betterment. Exceptionally it proves, for a time
ACNE 1047
at least, most intractable, relief being slow and often temporary. If
untreated, it frequently continues for several years or more, in the ma
jority of patients a spontaneous disappearance setting in as adult age
is reached. There are, however, many exceptions to this, and the state
ment that all cases are well by the time thirty is passed is not supported
by the experience of specialists. Many persist indefinitely, and especially
those of the indurated and dermic abscess type, and more particularly
acne of the back. Scarring, more or less permanent in character, re
mains in some instances. To a great extent it may be said that cure de
pends upon a recognition of the predisposing cause or causes and their
removal or modification.
Treatment.—Both systemic and local treatment are essential
in most cases; in patients approaching full maturity, and showing a
tendency to spontaneous disappearance, local applications alone will
often suffice. In many instances, however, constitutional medication
is of greater importance for permanent effect and should rarely be
omitted.
To secure the best results each case must be studied carefully and
all possible etiologic elements considered. Constitutional treatment
must be selected according to the predisposing influences in the individual
patient, remembering that digestive disturbances and constipation are
the most common causative factors. The value of exercise in the open
air, calisthenics, bathing, and other hygienic measures cannot be over
rated. Free bowel action is of essential importance. The diet should
be regulated, the food being plain but nutritious. All indigestible or
questionable foods are to be interdicted, especially those leading to fer
mentative indigestion. For dyspeptic patients and for those whose di
gestion is weak or capricious, bitter tonics, alkalis, nux vomica, acids,
pepsin, pancreatin, and saline and vegetable laxatives are to be variously
prescribed. Of the laxatives, cascara sagrada, the ordinary aloin-
strychnin-belladonna pill, rhubarb root, gray powder, calomel, Hun-
yadi János, Friedrichshall, and similar waters deserve special mention.
A mixture composed of ½ to 2 drams (2.-8.) of sodium benzoate or sodium
bicarbonate, 2 drams (8.) of tincture of nux vomica, 2 to 4 drams (8.-16.)
of fluidextract of cascara sagrada, and tincture of cardamom to make up 3
ounces (96.), of which a teaspoonful is to be taken after each meal,
can often be prescribed with advantage. Another combination often
of service and in very general use is a saline tonic, known usually as
the “mistura ferri acida,” made up of 1 ounce (32.) of magnesium sul
phate, 4 to 8 grains (0.25-0.5) of iron sulphate, 1 to 2 drams (4.-8.)
of dilute sulphuric acid, and mint-water to make 4 ounces (128.), of
which a tablespoonful is given in a full tumbler of water about twenty
minutes before breakfast. If the dose of this latter should not prove
laxative, it can be given also in the evening upon retiring; or, and ordi
narily to be preferred, 2 or 3 drams (8. or 12.) of sulphur can be added.
In chlorotic and anemic patients preparations of iron and arsenic
are useful, but the dose should be small, inasmuch as a large dosage of
these drugs is likely, by tending to disturb the digestion, to aggravate
rather than relieve. Arsenic has no specific value in acne, nor has sul-
1048 DISEASES OF THE APPENDAGES
phur internally the value popularly given it; calx sulphurata also has
failed to meet expectations, and is scarcely employed in this disease
at the present day. In debilitated subjects, and in those of strumous
habits, and of pale, pasty-looking skin, cod-liver oil, in doses of from ½
to 1 teaspoonful three times a day, is often a remedy of great value,
particularly in the sluggish atrophic, indurated, and dermic abscess
types. In those cases of acne in which the congestive element is marked
ichthyol has been commended.
Vaccine Treatment.1—Recently Wright and others have claimed
good results from injection of staphylococcic vaccine; dosage and
frequency were to be based upon the opsonic index of the blood.2
Others have noted only slight value from this vaccine, believing this to
be due to the fact that it is not the staphylococcus, but bacillus acnes,
that is the active organism in the production of the disease. Some phys
icians who still consider the staphylococcus of some etiologic import
employ a vaccine made from both these organisms. Fleming, Western,
Morris and Dore, King Smith, and others, believing some cases solely
due to the staphylococcus, some to the acne bacillus, and some to a
mixed infection, have employed the corresponding vaccine in the treat
ment, with alleged gratifying results. Many investigators, among whom
are Gilchrist, Fleming and Engman, have, however, in the past several
years been employing a vaccine made from the acne bacillus only with,
it is claimed, fairly uniform success. On the other hand, some careful
observers who have tried the vaccine treatment in acne cases, have not
been so fortunate in their results, but one at all observant must concede
that occasionally the result of such treatment seems strikingly rapid
and brilliant. Most conservative men look upon it as yet simply as an
adjuvant or an additional remedy, to be tried in extreme or persistent
cases in which the usual methods fail. Possibly, as Engman and others
believe, lack of uniform success with treatment is, in a measure at least,
rather due to our still imperfect knowledge of the technic, than to the
method itself.3 An autogenous vaccine is generally thought to be pref-
1 For literature references see under Etiology.
2 This study of the index is too tedious and uncertain except in the hands of a trained
expert; and it is now generally believed that it can usually be dispensed with, the
effect of one or two trial doses giving sufficient indication of frequency and quantity.
3 Engman, who is most enthusiastic in its use, advises the following technic:
After a dose of 3,000,000 to 5,000,000, one or two new lesions will appear within forty-
eight hours, generally the next day; if more than three appear during this negative
phase the dose is too large. About seventy-two hours after the injection the come
dones are expressed and all the lesions opened. The manipulation at this time brings
the immunizing blood to the part, since it is at the height of the “tidal wave of im
munity.” The large cystic lesions are opened by a thin cataract knife and the pus
squeezed out; the walls of the lesion are in this way rubbed together and by irritating
them fresh immunizing lymph is brought into the cavity. This method dries them up
within a few days. The patient is also instructed to apply hot towels to the face twice
daily for five minutes, so as to cause a local hyperemia. On the fifth to the seventh
day new lesions will appear, which signify another stage of depression, and are the indi
cation for a second dose of vaccine. Another dose of 3,000,000 to 5,000,000 is given; in
this way a cure is completed. Small doses sufficient to cause a short negative phase,
beginning with about 3,000,000, seem with us to be the best method. After several
doses new lesions cease to appear. If, after a few doses, new lesions appear after the
third day, a larger dose of 7,000,000 to 10,000,000 should be given, but this is rarely
necessary.
ACNE
1049
erable, nevertheless quite a number of experienced investigators have
failed to see much difference in action between this and the stock vaccine.
Local or external treatment is of essential importance in the man
agement of acne. The remedies used are of antiseptic character. There
are three methods of medication—by powders, by lotions, and by oint
ments. It will usually be found that no one method of application can
be used satisfactorily in a given case without occasionally having re
course to another. The ordinary case will, as a rule, demand for a suc
cessful issue a change from lotion to ointment or vice versâ. The method
of medication with powders is less efficient and least commonly em
ployed. Upon the whole, the method of treatment by lotions is the most
generally satisfactory, intermitting at times, and using an ointment.
The action of remedies is enhanced by thorough application. Powders
are to be dusted freely over the parts; lotions are to be dabbed on for
five or ten minutes, going over and over the affected region several times,
and allowed to dry; ointments should be carefully but thoroughly rubbed
in for several minutes or more, and the excess then be wiped off. What
ever the method of application selected, as soon as slight irritation or a
tendency to scaliness results, the remedy should be intermitted for one
or two nights, during which time a mild, soothing ointment, such as
cold cream or petrolatum, is to be applied, and all other measures omitted.
Scaliness is more frequently a result of the application of stimulating
lotions; salves produce at times redness and irritation, but unless pushed
or very strong, the grease constituent keeps the parts free from visible
epidermic exfoliation. Believing that seborrhea of the scalp, especially
the oily variety, is probably by extension a factor in some cases of acne,
when such is visibly present, it is a good plan to give it some attention,
more particularly as to shampooing every five to ten days, using the
medicated soap tincture for this purpose.
There are certain general directions as to the local management.
The affected part, usually only the face, is to be washed with a mild
toilet-soap, or in extremely sluggish cases with green soap or the tinc
ture of green soap instead of the toilet-soap; in indolent types the soap
tincture can be medicated with 10 grains (0.065) or more of resorcin to
the ounce (32.). The parts are then to be thoroughly rinsed and sponged
for from five to ten minutes with water as hot as can be comfortably
borne, wiped dry, and then the remedial application made. These
procedures are best carried out at night, in the morning washing with
tepid water. In severe cases, in patients desiring a rapid impression to
be made, this treatment may be repeated night and morning, or even three
times daily, until the parts are considerably irritated or roughened,
or even pushed to moderate scaliness, and then soothing remedies are
applied for a few days. When such an active method is employed, the
patient should, especially if the weather be cold and windy, be more or
less confined to the house, or an eczematous dermatitis may be brought
about. In addition to these preliminary and adjuvant measures, the
blackheads are, as far as practicable, to be removed. This may be
accomplished by the patient by pressure with the finger-ends or with a
watch-key-like instrument procurable in the shops, or best by the phys-
1050
DISEASES OF THE APPENDAGES
ician, and much more easily and satisfactorily with a fenestrated curet-
shaped comedo extractor. Opening the smaller pustules is not essential,
and even many of the larger pustules will care for themselves, but the
treatment is materially aided by puncturing or incising such lesions and
pressing out the contents. The cavity of the indurated lesions can be
touched with carbolic acid; or these and the dermic abscess type can be
washed out with a weak carbolic solution or with hydrogen peroxid.1
G. H. Fox has been a strong advocate in sluggish cases, in which the
lesions are somewhat superficial, of putting the skin on the stretch and
scraping it with the blunt-edged curet, using more or less pressure, thus
mechanically breaking and evacuating the pustules and removing many of
the comedones; considerable temporary disfigurement and irritation
follow, which may be allayed by soothing applications.
The remedial applications must, of course, vary somewhat in strength
and character with the local conditions. Thus, in cases in which the
lesions are acute, markedly inflammatory, hyperemic, tender, and pain
ful, milder applications, such as are of a soothing nature, are called for;
the boric acid lotion, calamin-and-zinc-oxid lotion, and similar lotions
used in eczema may be temporarily used. One of the most satisfactory is
composed of 40 grains (2.65) of calamin, 80 grains (5.35) of zinc oxid, 1
dram (4.) of boric acid, and water to make 4 ounces (128.); to this, if
the skin is very dry, can be added 2 to 8 minims (0.13-0.5) of glycerin.
Later, when the inflammatory aspect has abated, the addition of 4 to 20
grains (0.27-1.33) of resorcin is advantageous. In the average patient,
however, the eruption has usually been of some duration, and the lesions
are, comparatively speaking, somewhat sluggish, and will demand, even
at the start, remedies of a slightly or actively stimulating character.
The most valuable remedy in the external treatment of acne is sul
phur or its compounds, and it can be used in most of the cases with
variable advantage, sometimes slight, oftener pronounced; in some
patients, however, the skin does not bear it well, and irritation results;
in others, for some unexplained reason, the follicular openings blacken,
and the comedo element of the case becomes more conspicuous; in others
again the remedy has no effect whatever. In mild types sulphur may be
used as a dusting-powder, either alone or mixed with an equal part of
boric acid; it is not, however, very energetic when thus employed. The
most commonly prescribed sulphur lotion, and one that is often extremely
serviceable, is the following, known to most dermatologists as “lotio
alba”:
R. Zinci sulphat.,
Potassii sulphuret., ää gr. xxx-3iv (2.-16.);
Aquæ, 3iv (128.).
The most frequently prescribed strength is 1 dram (4.) each of the
salts, and when in this proportion and properly prepared, the sediment
which forms will constitute about one-fourth the bulk; when shaken,
1 While it is my experience that puncturing and incision of the lesions are helpful,
there is more risk of slight markings being left when this method, especially incision,
is employed than if the process is left to nature.
ACNE
1051
the lotion is milky in appearance, hence the name; it is entirely free
from odor. It seems difficult to have it properly made, due doubtless
to a deteriorated or a dried-out potassium sulphuret. The weaker
strength is prescribed in irritable or markedly inflammatory cases;
the strongest when the others have failed to make an impression. If
too drying, 1 or 2 minims (0.065-0.133) of glycerin can be added to
the ounce (32.). This lotion may be made still stronger, and in sluggish
cases more efficient, by having of the zinc sulphate 6 to 20 grains (0.4-
1.33) in excess of the potash salt, and by adding resorcin, 20 to 100
grains (1.3-6.6) or more, to the 4 ounces (128.). Sulphuret of potassium,
used alone in lotion form, is also of service, but its odor is disagreeable
and cannot be entirely disguised; it is prescribed as follows: 20 to 40
grains (1.33-2.65) of potassium sulphuret, 2 drams (8.) cologne water, 1
dram (4.) of benzoin tincture, and water to make 4 ounces (128.); after
solution of the salt, filtering. A lotion containing precipitated sulphur
4 drams (16.), glycerin 20 to 40 minims (1.35-2.65), alcohol 1 or 2 drams
(4. or 8.), with 4 ounces of water (128.) is also of value. Another sulphur
application (Kummerfeld’s lotion) of which I can speak highly is that
composed of 4 drams (16.) of precipitated sulphur, 10 grains (0.65) of
powdered camphor, 20 grains (1.35) of powdered tragacanth, and 2
ounces (64.) each of lime-water and plain water; if well prepared, this
is of somewhat thick, creamy consistence, and when applied makes a
good coating. There remain to be mentioned two other sulphur lotions
which have proved valuable in my hands, and also in the experience of
other specialists: R. Sulphur, lot., 3iv (16.); ætheris, f3iv (16.); alcoholis,
q. s. ad f3iv (128.). This is often useful in those cases of indurated
and sluggish type, and especially when there is a good deal of oiliness.
The other is the liquor calcis sulphuratæ; this should be diluted at first
with 10 to 15 parts water, and then rapidly increasing its strength accord
ing to circumstances, even up to the pure solution; it is more particularly
useful in sluggish, indurated, and dermic abscess cases.
Sulphur, usually the precipitated, is also used in ointment form,
and in some cases, although a small minority, it acts better than the
lotions; it is prescribed in the strength of 1 to 2 drams (4.-8.) to the
ounce (32.) of benzoated lard. The English are fond of an ointment of
hypochlorid of sulphur, a dram (4.) to the ounce (32.) of lard.
Another sulphur-containing salve which often proves beneficial is
made as follows: ½ dram (2.) of potassium sulphuret is dissolved in
1 dram (4.) of water, and to this is added ½ dram (2.) of zinc sulphate,
and allowed to react; it is then stirred until the sulphureted hydrogen
odor entirely disappears, and finally rubbed up with 2 to 4 drams (8.-16.)
of cold cream or cold cream and lanolin.
In recent years ichthyol has been added to the therapeutics of acne,
and is often useful. It is employed in lotion or ointment form, usually
the latter; as an ointment, 1 to 3 drams (4.-12.) to the ounce (32.) of
equal parts of simple cerate and rose-water ointment; or as a lotion,
about the same strength with water. It seems to be more especially
valuable in acne of a pustular and pustulotubercular type, and in the
latter its application as a 25 per cent, plaster is often advantageous.
I052
DISEASES OF THE APPENDAGES
A compound ointment containing both sulphur and ichthyol is also of
value:
R. Sulphuris præcipitati, 3ss-ij (2.-8.);
Ichthyol, 3j-ij (4.-8.);
Adipis vel petrolati, q. s. ad 3 j (32.).
In extremely sluggish cases this same ointment with 1 or 2 drams (4.-8.)
of green soap (sapo viridis) to the ounce (32.) will act more energetically;
in fact, sapo viridis may be incorporated in any of the ointments named
if a more positive action is desired.
Resorcin as a lotion, from 5 to 30 or more grains (0.32-2.) to the ounce
(32.) of water, or of water and alcohol, is a clean and often useful appli
cation. It should be cautiously used at first in the stronger proportions,
as exceptionally it provokes an eczematoid dermatitis, especially if used
in salve form. Boric acid is likewise valuable, either as a strong alco
holic lotion or as a combined lotion with resorcin. The following has
been of service:
R. Resorcini, 3ss-ij (2.-8.);
Acidi borici, 3j-ij (4--8.);
Zinci sulphatis, gr. xx-xxx (1.3-2.);
Alcoholis, f3ss (16.);
Aquæ destillatæ, q. s. ad f3iv (128.).
The lotion of calamin and zinc oxid, already referred to, is often of service
in the more stubborn inflammatory types, if strengthened with resorcin,
5 to 20 or more grains (0.35-1.35) to the ounce (32.).
Salicylic acid is a remedy for occasional trial in obstinate cases, from
10 to 60 grains (0.65-4.) to the ounce (32.) of ointment, but is often used
as an addition—from 10 to 20 grains (0.65-1.3) to each ounce (32.)—
to the other ointments already named; it is to be observed that the addi
tion of this ingredient renders any ointment more active.
As already remarked, sulphur preparations are sometimes without
effect, or after a time fail to influence the eruption. In such instances,
and also in others, the mercurials are not infrequently prescribed. Cor
rosive sublimate is the most valuable, and is usually the active agent in
almost all the patent toilet lotions. It is, of course, to be specially noted
that in changing from a sulphur to a mercurial application or the reverse,
several days should be allowed to intervene, or else there occurs a tem
porary slight staining of the skin from the formation of black mercuric
sulphid; the disfigurement showing itself more especially by a darkening
at the sebaceous gland outlets.
Corrosive sublimate is employed as a lotion, from ¼ to 4 grains
(0.016-0.25) to the ounce (32.) of water, or of water and alcohol; and
such a lotion is materially strengthened by the addition of from 3 to 8
grains (0.2-0.5) of zinc sulphate to each ounce (32.). The following is a
formula frequently used: R. Hydrargyri chloridi corrosivi, gr. ij-xij
(0.16-0.8); zinci sulphatis, gr. xx (1.3); tincturæ benzoini, f3ij (8.);
aquæ, q. s. ad f3iv (128.); mix and filter. Calomel and white precipi
tate ointments, 3 to 10 per cent, strength, are also at times of service, and
may often be alternated with the corrosive sublimate lotion.
ACNE
I053
Acne of the back or trunk is, upon the whole, treated with the
same preparations as that of the face, but much more energetically,
and usually with stronger applications. Green soap or tincture of
green soap washing daily, followed by the remedial application, and
then a dusting-powder of powdered boric acid, with 20 to 30 grains (1.35-
2.) of salicylic acid to the ounce (32.), is valuable. Liquor calcis sul-
phuratæ is a useful application in some cases of acne of this region.
Resorcin in strong solution—up to 1 dram (4) to the ounce (32.) of equal
parts of water and alcohol—sometimes acts with energy. A fairly sat
isfactory method in many hands has been with formalin, using this
at first much diluted, but finally in sufficient strength to produce con
siderable irritation or a mild dermatitis, the plain boric acid powder
being used as a dusting-powder. The daily use of a compound dusting-
powder (C. N. Davis), consisting of about \ dram (2.) of precipitated
sulphur, about 10 to 20 grains (0.66-1.35) of powdered camphor, and
boric acid or boric acid and talc to make the ounce (32.), has also proved
markedly beneficial in some cases. The undershirt should be changed
often and boiled or washed, then put in boric acid or weak formalin
solution and dried.
The various plans here outlined will usually suffice for most cases
of acne, but in some, where more rapid action is desired and when pa
tients remain at home or are in the hospital, the exfoliating pastes or
salves can be used. The following are the pastes that are most com
monly employed for this purpose: R. Beta-naphthol, 3ss-ij (2.-4.);
precipitated sulphur, 3iv (16.); sapo viridis, 3ij (8.); and rose-water
ointment, 3ij (8.) (Lassar); and R. Resorcin, 3ss (16.); zinc oxid, 3j (4.);
terra silicea, gr. xij (0.7); benzoated lard, to 3j (32.) (Unna, Isaak).
This is smeared thickly on the face, and is best applied spread upon lint;
it is kept on for fifteen to thirty minutes, and then rubbed off with a
piece of linen or absorbent cotton greased with oil or cold cream, and then
the parts washed with warm water and soap, followed with soothing
applications, such as cold cream, vaselin, or talcum powder. It is re
peated every night or oftener if necessary, and in a few days sufficient
dermatic irritation has been excited, and is followed by desquamation.
Repeated applications, two or three times daily, of a 25 to 50 per cent,
alcoholic solution of resorcin act promptly and satisfactorily in some cases
in bringing about exfoliation; Bronson has also found this plan efficient.
In the use of these peeling applications, as soon as the exfoliation and
irritation have disappeared, the treatment is again repeated, and so on
until the result is obtained.
As with many other skin diseases, the Röntgen rays have been used
in this, and sometimes with brilliant results. I can add my indorse
ment of its value. Many cases can be managed just as well without it.
I reserve it for persistent, rebellious cases, and even in these instances
employing it, at intervals of a week or ten days, as a supplementary meas
ure to other treatment. A soft to medium tube is used. The exposures
should be made cautiously, at 10 to 15 inches distance, and for three
to four minutes duration, and later, if necessary, five to ten minutes.
It is best not to push its use to the point of reaction, as in some instances,
1054 DISEASES OF THE APPENDAGES
when too much action is brought about, and exceptionally in other
instances, and sometimes even after but a few short irradiations, dark
freckles result; and occasionally (especially if treatments extend over a
long period) a tendency to an atrophic, old-age, somewhat wrinkled con
dition of the skin. Down is also sometimes, according to patients’
statements, produced, but I am not convinced of this. These blemishes
gradually lessen and disappear, except the atrophic wrinkled condition,
which, if pronounced, may remain to some extent. Eyes, eyebrows,
and scalp should be properly protected. The protecting box or casing
can be so arranged as to protect the scalp hair, a thin covered tin- or
lead-foil band can be placed over the eyes and eyebrows.1
Repeated applications of the high-frequency current, recently com
mended, have also been of service in some of my cases, and have sup
planted the faradic and galvanic currents; it is applied by means of a
flattened hammer electrode, and this is held 1/8 to 1/4 inch from the skin;
and the application should be sufficiently long-continued as to produce
moderate redness or reaction.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |