| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
1060 DISEASES OF THE APPENDAGES
ACNE ROSAŒA
Synonyms.—Rosacea; Gutta rosacea; Gutta rosea; Acne erythematosa; Fr.,
Acne rosée; Acné rosacée; Couperose; Ger., Kupferrose; Kupferfinne.
Definition,—A chronic congestive disease of the face, more com
monly limited to the nose or nose and immediate neighboring parts
of the cheeks, characterized by passive hyperemia, later by slight or
marked capillary dilatation and enlargement, and frequently by more
or less acne or acne-like lesions, and in some instances tissue hyper
trophy.
Symptoms.—The disease begins with slight passing redness of
the part, frequently the nose only at first; this appears after exposure
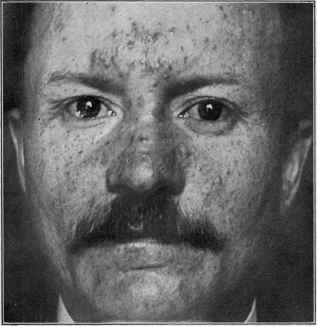
Fig. 264.—Acne rosacea of a not uncommon type, showing hyperemia, dilated capil
laries, and acne or acne-like lesions.
to cold or heat, or after hot drinks, or during an attack of indigestion,
or it may appear independently of any recognizable influence. The
condition subsides sometimes in minutes, sometimes in hours, or a day
or two. After a variable number of recurrences, or after weeks or a
few months, the hyperemia becomes persistent, showing aggravation
upon excitement, exposure, etc In color it is somewhat variable
between bright and dull red, sometimes with a venous tint. A slight
or marked oiliness of the nose is frequently to be noted; also sometimes
enlarged gland openings. Later, upon close examination, permanently
dilated capillaries, several or more in number, can be seen, especially
toward the alæ. The redness is of slight degree or quite pronounced,
ACNE ROSACE A
1061
disappearing entirely upon pressure; and the part is somewhat colder to
the touch than normal. This condition, representing what is usually
described as the first stage of acne rosacea, may persist as such, varying
slightly in degree, but with little if any tendency to extension or to
tissue hypertrophy.
In most cases, however, and often conjointly with the earliest ap
pearance of the passive hyperemia, acne and acne-like papules, nodules,
and pustules, at first few, later in numbers, may show themselves. Not
infrequently the neighboring part of the face within the malar promi
nences also exhibits the eruption; and in some instances the middle part
of the forehead and the chin are likewise the seat of hyperemia and
acne lesions. This area—a long oval with the chin and middle forehead
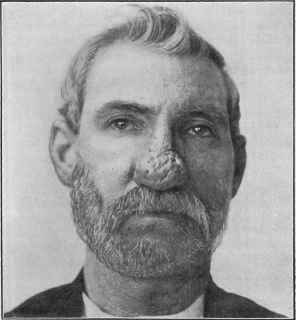
Fig. 265.—Acne rosacea (rhinophyma) showing marked hypertrophy.
as the end boundaries and the malar bones as the side boundaries—
is that beyond which acne rosacea seldom extends to any great degree;
it may, however, sometimes present over the entire face; and in extreme
cases, especially in heavy drinkers and those with an associated derma
titis seborrhoica, even the bulbar conjunctiva may exceptionally show
a suffused redness, suggestive of telangietatic points, and a few superficial
phlyctenule-like lesions.1 With the acne lesions there is usually noted,
about the nose especially, enlarged gland-ducts containing oily or semi-
solid sebaceous material, and in occasional cases a slight tendency to mild
1 Holloway, “The Ocular Manifestations Associated with Acne Rosacea, with the
Report of a Case of So-called Rosacea Keratitis,” Arch, of Ophthal., 1910, vol. xxxix,
No. 4 (with review of the subject and references).
1062
DISEASES OF THE APPENDAGES
seborrheic dermatitis. The enlarged capillaries become more numerous
and may be seen on all affected parts, more especially, however, the nose
and closely adjacent skin. In this picture is to be found what is usually
described as the second stage of the disease, and it rarely, as observed
in this country at least, goes beyond this. It varies somewhat, and may
measurably improve under favorable conditions. The pustular lesions
are somewhat or wholly like those seen in ordinary acne, but the papules
or nodules, especially about the nose, seem more like tissue indurations,
and the suppuration in the pustule is usually close to the surface and
rather slight.
In exceptional instances the disease advances; somewhat soft tissue
hypertrophy, diffused or nodular in character, is noted on the nose,
more especially toward the end and at the alæ; the glandular openings
are large, the blood-vessel hypertrophy more marked, some small vari-
cosities occasionally presenting, and the whole organ is slightly or con
siderably enlarged, constituting the so-called third stage of the disease.
The same characters are usually to be seen, but to a less degree, in the
immediately neighboring skin; it is only exceptionally that distinct
hypertrophic tissue changes (other than vascular) are noted elsewhere
on the face, usually about the middle forehead and chin. In some of
these hypertrophic cases the disease is limited to the nose region, in
others there may in addition be seen on other parts of the face the acne-
like lesions and telangiectases of the more common type. In rare in
stances the hypertrophy of the cutaneous and subcutaneous tissue of the
nose assumes disfiguring or even immense proportions, and presents
more or less lobulation, and, in extreme cases, pendulous masses—
rhinophyma. In these hypertrophic types the color is often a deep red
or purplish red.
As a rule, there are no subjective symptoms, although there are
at times, in those cases in which acne lesions are numerous, some ten
derness and soreness, and exceptionally, more particularly in those ex
hibiting a tendency to seborrheic dermatitis complication, slight itching.
Etiology.—Acne rosacea furnishes about 3 per cent, of all skin
cases—a less relative proportion in dispensary practice than in private
practice. It is closely allied to acne in its etiology, except as to the
age at which it is observed; the former is not commonly seen before
the thirtieth year, and most of the cases observed earlier are usually
of the nose, and associated with or clearly a part or consequence of
oily seborrhea of that organ. The disease, in its milder grades, is
thought to be more common in women, although I think not so much
so as is generally believed; women, being more sensitive to facial dis
figurement, seek advice more frequently. The hypertrophic form is
rarely seen in women. Disturbance of the digestive apparatus must be
considered the most important etiologic element in the large majority
of patients, and such disturbance may be due to improper food or im
properly cooked food, excessive indulgence in alcoholic drinks, tea, and
coffee, etc. A feeble circulation, debility, and gouty diathesis seem also
to be of influence. Inordinate use of tobacco is a possible factor. In
addition to this indirect action of alcohol, it has also the effect of produc-
ACNE ROSACEA
IO63
ing peripheral vascular dilatation, and its free use is responsible for many
cases, and doubtless for almost all of those of marked hypertrophic de
velopment. It is by no means, however, as many are inclined to believe,
the sole cause of the malady, for not infrequently it is met with not only
in those of temperate habit, but in total abstainers, even rhinophyma
having been observed in the latter (Hebra, Jr.). In women a not unim
portant factor is functional or organic uterine disorder, and in such, as
well as in others of this sex free from this element, the disease usually is
worse at and preceding menstrual periods. Another cause or con
tributory factor in some cases is to be found in intranasal pressure or
disease (Seiler, Brocq, Bergh, Sticker), giving rise to vascular and lym
phatic obstruction. Inflammation of the hair-follicles (sycosis) just
within the nares, by producing constant hyperemia of the integument,
also tends to lead toward the disease (Jarisch, Elliot). There are also
external factors in many cases, such as lack of cleanliness, cosmetic and
other irritants, exposure to cold winds, as with drivers, cabmen, etc.,
great heat, and the rays of the sun. In some patients a seborrhea pre
cedes or is seen in the course of the disease, and may in some cases have
etiologic importance. Unna gives this factor a high place, or rather con
siders the malady in many instances a seborrheic catarrh, giving it the
name rosacea seborrhoica. With others (Jarisch, Hallopeau, Leredde,
and others) I believe the seborrheic condition is often secondary.
Pathology.—The first stage in acne rosacea is a hyperemia,
probably angioneurotic (Eulenberg, Simon, Auspitz), but in some cases
in consequence of a seborrheic process. In consequence of the persistent
hyperemia and irregular periodic aggravations the vessels. become per
manently enlarged, and there is induced in many cases a slight hyper-
nutrition of the skin, which has as a result variable hypertrophic changes.
The sebaceous glands become involved, nodules, first of a gelatinous and
later fibrous character, and acne or acne-like lesions are usually super-
added, either secondarily or as a part of the pathologic process. The
pathologic anatomy has been studied by many observers (Simon, Biesia-
decki, Hebra, Jr., Leloir and Vidal, Rokitanski, Piffard, Elliot, Dohi,
and others).1 The markedly hypertrophic forms are especially due, in
addition to the above, to connective-tissue growth and enlargement of
the sebaceous glands. There is usually noted in the third stage a pro
nounced hyperplasia of the dermic connective-tissue elements. The
increased vascular dilatations are partly the consequence of the chronic
hyperemia, and partly doubtless to a blocking-off of some of the return
vessels from cicatricial formations resulting from follicular suppuration
and destruction. In some of the enlarged vessels the walls are thinned,
in others thickened, with considerable surrounding connective-tissue
hypertrophy. The veins show enlargement, and sometimes resemble
cavernous tissue (Leloir and Vidal). The acne or acne-like lesions are,
for the most part at least, similar to those of ordinary acne, to which
disease it certainly seems to bear relation, although this is of late denied
1 Piffard (Wagner’s paper), Archives of Clinical Surgery, 1876-77, vol. i, p. 21;
Hebra, Jr., Archiv, 1881, p. 603 (with histologic plate and review of literature with
references); Dohi (2 cases), ibid., 1896, vol. xxxvii, p. 371.
1064 DISEASES OF THE APPENDAGES
by others who consider that the nodular and pustular lesions are wholly
different from those of the latter malady.
Diagnosis.—The diagnostic characters are the redness, dilated
capillaries, and, at times, the connective-tissue and glandular hyper
trophy, with, in most cases, acne lesions superadded; the limitation
to the face, especially the region of the nose, or nose, chin, and middle
forehead; the evident involvement of the sebaceous glands in most in
stances; the absence of ulcèrative tendency and the history of the case—
these are points of difference which will usually serve to distinguish it
from acne, erythematous eczema, dermatitis seborrhoica, lupus erythe-
matosus, tubercular syphiloderm, and lupus vulgaris.
The distinct hyperemic element is wanting in ordinary acne; its dis
tribution is irregular and general over the face; there are, in most in
stances, numerous comedones, and there is no dilatation of the vessels,
and, as a rule, its subjects are younger. Erythematous eczema is never
limited to the acne rosacea region, the skin is somewhat inflammatory
and infiltrated, with usually slight or moderate scaliness, and trouble
some subjective symptoms, and no dilated vessels, and a different his
tory. Dermatitis seborrhoica is frequently seen in this region, but it is
a distinctly oily or scaly disease, with no blood-vessel dilatations, and is
ordinarily associated with a seborrhœa capitis; there is often variable
itching or burning. Lupus erythematosus is sharply defined, with, as
a rule, an elevated border; there is slight or moderate scaliness, a tend
ency to central thinning, and atrophy. Both the tubercular syphilo-
derm and lupus vulgaris may bear slight resemblance to the hypertrophic
nodular acne rosacea, but they generally tend to ulcerative action and
scarring or to atrophic change; lupus vulgaris usually begins in early
life, and the lesions of the syphiloderm almost invariably are noted to be
circinate or segmentally grouped; dilatation of the capillaries is not an
essential feature of either, and the history is different in both diseases. ’
Prognosis.—The disease is obstinate, but all cases are favorably
influenced by treatment; the mild and moderately developed types,
under proper management, with the cordial and persistent coöperation
of the patient, are usually curable, several months, and sometimes longer,
being required, progress toward recovery being more rapid at first.
The removability of the etiologic factors will naturally have much to do
with the character of the prognosis given, both as to immediate relief
and freedom from recurrence. The hypertrophic forms admit of im
provement, and even in those of extreme development much can be
accomplished and the disfigurement materially reduced by surgical pro
cedures.
Treatment.—In great measure this is, excepting as to the dilated
capillaries and connective-tissue hypertrophy, closely similar to that
of acne, both as to its constitutional management and local medica
tion. Considering the possible etiologic factors mentioned, the chief
attention is to be directed to supervising the diet, improving the diges
tion, a free action of the bowels, and the avoidance of the predisposing
and exciting influences. In women inquiry is to be made as to the men
strual function and as to possible functional or organic uterine disease.
Acne rosacea
1065
The diet should be plain but substantial, especially avoiding all indi
gestible food, such as mentioned under Acne; the avoidance of more than
slight indulgence in tea, coffee, and cocoa, especially the first named,
and the absolute prohibition of alcoholic drinks in any form. The use
of tobacco should also be kept within moderate limits. As there are
no special remedies, the constitutional treatment, if called for, is to be
based upon a correct appreciation of the etiologic factors in the individual
case, digestives, laxatives, tonics, and cod-liver oil being most usually
prescribed. The morning saline mixture and the compound cascara
mixture to be found under Acne are often of service in those constipated
and of weak digestion. In the latter a prescription of hydrochloric acid,
strychnin, and pepsin is also of value, along with the daily or occasional
administration of a laxative. Ergot and ichthyol are two drugs which
have some support for internal administration in this disease, the former
in 20- to 60-minim (1.35-4.) doses, and of the latter (Unna, Morris, and
others) 3 to 10 minims (0.2-0.7) three times daily, but I have not been
able to get the good from their use that others have.
The external treatment of the earlier stages and the hyperemic and
inflammatory lesions of acne rosacea are, as already stated, very similar
to that of acne. Any existing intranasal pressure or follicular inflam
mation or a seborrhea should receive attention. The same general
directions as to preliminary measures, such as the soap-and-water wash
ing and hot-water sponging, are to be advised; occasional cases in which
the slightly scaly seborrheic element is more or less pronounced, as a
rule, only admit of the sparing use of soap, which in these and in all
others should be employed at night. Massage is not advisable. While
the remedial applications are those employed in acne, there are, however,
several of these which, in my experience, are more generally useful than
others. In the cases of considerable hyperemia and of widespread
distribution of an irritable type, and in which acne lesions are somewhat
numerous, a most admirable beginning application is that of the calamin-
zinc-oxid lotion. This is to be dabbed on freely and allowed to dry on;
in the morning the parts washed off according to the usual custom of the
patient, and the lotion again applied; if the patient goes out, the powder
which dries on can be gently wiped or rubbed off. Or in the morning
a plain talcum powder, made skin color by the addition of a few grains
(fractional part of a gram) of calamin to the ounce (32.). Resorcin added
to this lotion, 1 to 5 or more grains (0.065-0.35) to the ounce, increases
its strength. This treatment is to be continued as long as it materially
benefits, and then recourse be had to the lotion of zinc sulphate and potas
sium sulphuret, each 20 grains to 2 drams (1.35-8.) to the 4 ounces (128.)
of water. In many of these irritable cases this wash can be used from the
beginning in the weakest strength, and gradually increasing if it does
not irritate. Very often this lotion with 1 minim (0.065) of glycerin
to each ounce (32.) will add to its permissibility in irritable types. Later,
and in sluggish cases, alcohol, ½ to 1 dram (2.-4.) to the ounce (32.),
can be added to advantage, and in such cases very often the preparation,
when improvement begins to lag or ceases, can be rendered more active
and again beneficial by having an excess of 2 to 6 grains (0.13-0.4) of
1066
DISEASES OF THE APPENDAGES
zinc sulphate over the potassium salt in each ounce (32.). Very often
the plan of using the calamin-zinc-oxid lotion in the morning and the
stronger wash in the evening has served me well; or they can be used on
alternate nights. If irritation or slight scaliness ensues, the wash can
be used at night and cold cream in the morning, wiping it off on going
out.
Another application which is especially useful in many instances is
the Kummerfeld lotion, formula for which is given under Acne; it should
be used at night freely, and several times daily when possible, and occa
sionally intermitted if roughness or irritation of the skin results; or now
and then replacing it with an application of cold cream or with the cala-
min-zinc-oxid lotion. In this disease, too, probably even more than in
acne, the liquor calcis sulphuratæ (Vleminckx’s solution)1 will be found
of benefit, using it diluted with 10 to 15 parts of water at first, and
rapidly increasing in strength until irritation or trifling exfoliation is
produced, and then reducing slightly and continuing, intermitting oc
casionally, if necessary, as with other lotions referred to. In those
cases in which there is considerable oily seborrhea the sulphur-ether-
alcohol lotion (see Acne) is often more serviceable. Other lotions re
ferred to in treating acne can also be tried from time to time in obstinate
types in which the above are without result or cease to benefit. In this
disease, as in many others, an application benefits for a time only, and
then is to be set aside; its resumption later will often again prove of value.
Ointments are not so generally useful as lotions, although progress
is more rapid in some cases when one temporarily gives place to the
other. They are to be applied as described in acne. Precipitated sul
phur ointment, 30 grains to 2 drams (2.-8.) of sulphur to the ounce (32.)
of cold cream or benzoated lard, acts satisfactorily, for a time at least,
in some instances. The ointment made with a strong solution of zinc
sulphate and potassium sulphuret, referred to in Acne, is also sometimes
valuable and deserves a higher position ordinarily than the plain sulphur
ointment. Ichthyol (Unna and others), in ointment and lotion of 10
to 25 per cent, strength, is often of striking advantage in this disease,
but often fails to make an impression, and exceptionally aggravates;
and it is difficult to say in what particular case its best effects are to be
expected; probably in those of markedly hyperemic type, and in which
suppurative lesions are numerous. It will often act more satisfactorily
as a lotion than as an ointment.
White precipitate and calomel ointments, 20 to 60 grains (1.35-4.)
to the ounce (32.) of ointment, have also had a place in the treatment,
but are, as a rule, much inferior to the applications already mentioned.
Corrosive sublimate lotions (see Acne) are at times of service. Mer
curial plaster kept applied (Hebra, Kaposi, Neumann) as constantly as
possible is often of value in cases in which somewhat hard nodular or
papular lesions are present. Ichthyol plaster, 25 per cent., is also of
service in such instances. Tannic acid, in lotion or ointment form, is
occasionally useful; the former, 5 to 60 grains (0.35-4.) to the ounce
(32.) of equal parts of water and alcohol, and the ointment, of 10 to 20
1 Stelwagon, “Vleminckx’s Solution in Acne Rosacea,” Med. News, July 7, 1883.
ACNE ROSACE A
1067
per cent, strength; the lotion is the more valuable. I have used it in the
type in which the disease was more or less strictly limited to the nose,
with some oily seborrhea and enlarged glandular openings. In this class
of cases, too, electrolysis, repeated every few weeks, freely used within
the openings and the interspaces, is an adjuvant of considerable value,
employing a current of 2 to 5 milliampères; it produces irritation lasting
a day or two, and the condition looks temporarily worse. Multiple
punctures with a sharp-pointed bistoury are also of value in these cases,
but probably no more so than electrolytic punctures; bleeding should
be favored by hot-water compresses, followed later by cold compresses.
The application of electricity (Cheadle, Piffard, and others) is sometimes
beneficial, the high-frequency current being the most valuable. It is
applied in the same manner mentioned in Acne. The Röntgen-ray treat
ment is another recent plan variously commended, and has sometimes
proved useful in some of my cases, especially in those of markedly dilated
and pustulous gland openings, and those of a hypertrophic character;
it is applied in the same cautious manner as in acne.
Under these plans, given above, the most disfiguring elements of
average cases—the diffused hyperemia and the acne lesions—can be
removed. There remain in many instances, however, the dilated ves
sels, and in a less number tissue hypertrophy, which require other treat
ment. The former can be destroyed either with the knife, cutting
transversely at several points, or cutting down their length; by a Paquelin
microcautery (Unna, Elliot), or preferably and most satisfactorily by
electrolysis (Hardaway and others).1 The electrolytic method is essen
tially the same as employed in the removal of superfluous hairs (q. v.);
the needle may, if the vessel is short, be inserted along its length, or if
long, may be inserted at several points in its course. It is usual to attach
the needle to the negative pole, and, upon the whole, this is the most
satisfactory, but in occasional rebellious cases I have used it attached
to the positive electrode, and found it sometimes effective; in the latter
instances a gold or iridoplatinum needle is to be used, for reasons stated
(see Hypertrichosis). The strength of the current required is from \ to
2 milliampères—about 2 to 6 or 8 wet cells and 3 to 12 dry cells. The
needle is kept in from several to thirty seconds, according to effect; the
blood is noticed to run up the vessel, and the latter thus apparently disap
pears, but as soon as the needle is withdrawn and the gases generated
are absorbed, the blood, if the vessel is long, returns part way; new
punctures are to be made in such. The appearance of a distinct blanch
ing at the point of insertion, enlarging to the size of a small pea, should
be a signal for withdrawal of the needle, otherwise too much action may
follow. Very often, from the resulting hyperemia after a series of punc
tures, the vessels, if at all near to each other, can no longer be detected,
and further operations must then be postponed. Hot-water applica
tions should be made immediately afterward for a few minutes, followed
by cold. The electrolytic procedure is to be frequently repeated until
the destruction of the vessels ensues. Unfortunately, there often exists a
tendency to new vessel-formation or dilatation.
1 Hardaway, Arch. Derm., 1879, vol. v, p. 356.
1068
DISEASES OE THE APPENDAGES
The slight connective-tissue hypertrophy can sometimes be re
duced by multiple punctures and scarification (Hebra, Neumann, Veiel,
Squire, and others) and by electrolytic punctures (Hardaway); whatever
the method, it must be frequently repeated. The moderately hyper-
trophic and also extreme cases I have sometimes been able to reduce
by electrolytic destruction, both by introducing the needle down into the
glands (Brocq) and through the skin between the glandular openings,
using a current of 3 to 6 milliampères—about 4 to 10 wet cells, and 6 to
20 dry cells—and allowing the needle, attached to negative pole, to re
main in for twenty to forty seconds, in order that slight destruction may
result and cicatricial contraction ensue. Minute galvanocautery punc
tures (Unna’s micro-Paquelin or galvanocautery) are also useful. Car-
bon-dioxid snow as a superficial cauterant could also be used in the
milder cases. In extreme cases of excessive connective tissue growth,
however, the most rapid and usually quite satisfactory treatment is by
ablation or decortication with the scissors or knife; the condition rarely
recurs.1
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |