| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
ACNE VARIOLIFORMIS2
Synonyms.—Tuberculide; Acne rodens (Vidal and Leloir); Acne necrotica (Boeck);
Lupoid acne; Necrotic granuloma (Johnston); Acné á cicatrices deprimée (Besnier
and Doyon); Folliculites cicatricielles nécrosiques (Hallopeau and Leredde).
Definition.—An eruption commonly characterized by lesions
of a moderately superficial, papulopustular type, discrete or grouped,
occurring most commonly on the upper part of the forehead and scalp,
sometimes on the extremities and other parts, and leaving scars some
what similar to those of variola; in other cases, especially those involving
other parts than face and scalp, the lesions may be solidly papular, fre
quently follicular, sometimes with an exfoliating scale.
This name was given by Hebra, and should not be confounded with
the similar name occasionally found in the French literature and applied
to molluscum contagiosum. In the class acne varioliformis, which in
my belief is representative of the tuberculides, are included therein the
various cases described under the names of acne necrotica (Boeck),
acnitis, folliclis (Barthélemy), necrosing folliculitis, impetigo rodens
(Devergie), Pollitzer’s hidradenitis suppurativa,3 acne urticata, Pro-
1 For details as to apparatus, technic, etc, see article on Radiotherapy in the chap
ter on General Remarks on Treatment; and for possible detrimental effects see x-ray
dermatitis; and also the illustration (Fig. 4) of its evil effects in Burnside Foster’s
paper, Jour. Cutan. Dis., 1909, p. 72.
2 References to the chief literature of this and allied diseases are to be found in
Bronson’s paper (“Notes on Certain Pustular Diseases Attended with Atrophy”), Jour.
Cutan. Dis., 1891, p. 122, and in Fordyce’s articles, ibid., p. 128, and (“A Contribution
to the Pathology of Acne Varioliformis Hebræ”), ibid., 1894, p. 152, (based upon 2
additional cases)—all with illustrations; also in Johnston’s paper (“The Cutaneous
Paratuberculoses”), Philada. Monthly Med. Jour., Feb., 1899; and in that by Löwen-
bach (“Acne Urticata”), Archiv, 1899, vol. lxix, p. 29. These several papers together
cover the important literature pretty fully.
3 Hidradenitis suppurativa: Verneuil, “Hydrosadenite phlegmoneuse et absces
sudoripares,” Arch. gén. de méd., 1864, ii, p. 537, 1865, i, p. 327; Pollitzer’s paper,
“Hydradenitis destruens suppurativa,” Jour. Cutan. Dis., 1892, p. 9, is the most impor
tant on this disease, and reviews the literature of similar or allied diseases, with refer-
ACNE VARIOLIFORMIS
1055
fessor Duhring’s small pustular scrofuloderm, acne agminata (usually
on face, with tendency to grouping), the acne necrotisans et exulcerans
serpiginosa nasi (folliculitis exulcerans serpiginosa nasi) of Kaposi (a
grouped and spreading papular eruption on the nose, undergoing necrosis
or purulent change, and leaving conspicuous scarring),1 and the acne
telangiectodes of Kaposi (vascular, sometimes lupus-like papules, in
termingled with acne on face, and frequently terminating in scar for
mation). Unna’s ulerythema acneiforme is also believed by Vidal,
Leloir, and others to belong to acne varioliformis. The essential char
acteristics of these various cases are usually discrete, sometimes ag
gregated, pin-head to pea- or bean-sized papules or nodules, slightly
elevated, rarely deep-seated, with somewhat flattened top, reddish in
color, underlying slight necrotic changes with consequent central depres
sion, and, as a rule, comparatively insignificant pus-formation, followed
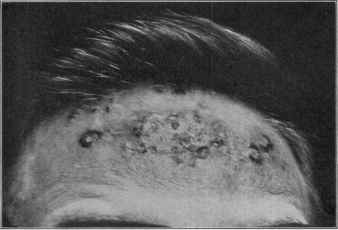
Fig. 262.—Acne varioliformis of a somewhat severe and grouping type (some lesions
scattered through the forepart of the scalp also),
by slightly depressed or varioliform scars. That there may be both
pathogenic and histopathologic differences is not improbable, but there
ences to date; and Barthélemy’s paper, “De l’acnitis,” Annales, 1891, p. 1 (disseminated
with colored plates), reads as if it were the same disease, and it is generally so considered,
but Barthélemy holds a contrary opinion; Dubreuilh, ibid., May, 1892, and Arch, de
méd. exper. et d'anat. patholog., Jan. 1, 1893 (2 cases, with review of literature and his-
tologic study). See also case reported by Bronson (acne varioloformis of the extremi
ties), Jour. Cutan. Dis., 1891, p. 121, and histologic examination by Fordyce, ibid., p.
128; and case, “An Unusually Extensive Folliculitis and Perifolliculitis: its Connection
with the So-called Tuberculides,” reported by Trimble, ibid., 1907, p. 256 (with case
illustrations and histologic cut).
1 Kaposi, “Ueber einige ungewöhnlichen Former von Acne,” Archiv., 1894, vol.
xxvi, p. 82; E. Finger, “Folliculitis Exulcerans Serpiginosa Nasi,” Wiener med. Wochen-
schr., Mar. 6, 1902, with review of the literature; Brandweiner (blastomycosis
and its relations to the folliculitis exulcerans serpiginosa nasi of Kaposi), Archiv,
1904, vol. lxxi, p. 49, reports a somewhat questionable case, presumably Kaposi’s disease
(with literature review), in which he found organisms, apparently blastomycetes, and, on
this scant foundation, is led to conclude that these two diseases are most probably iden
tical.
1056 DISEASES OF THE APPENDAGES
is a strong family clinical resemblance; their appearances and behavior
are much alike, their course more or less persistent and stubborn, the
scarring about similar in character, and the plans of treatment advised
essentially the same.1
Symptoms.—The eruption, which in average cases is rather
scanty, consisting usually of from ten to thirty lesions, begins by the
appearance of small pale-red maculopapules or papules, scarcely rising
above the surface; they gradually become larger and more elevated and
of a brighter red, which commonly, however, soon becomes dull red in
hue. In general the papule or small nodule is pierced by a hair, which
may be merely downy and scarcely perceptible, or on the scalp and other
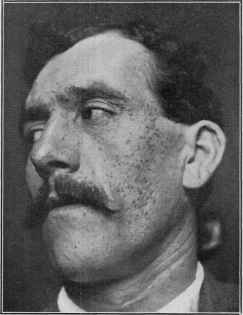
Fig. 263.—Acne agminata; six to eight months’ duration; showing some remaining
lesions and scars; stage of almost complete recovery.
hairy regions, as the face, it is one of the larger hairs; not infrequently,
however, it is entirely free from a hairy filament. The lesion is sluggish
in its course, and after reaching its acme, which requires several days to
a week or two, it often flattens, and the central part shows pustulation,
1 Crocker, Brit. Jour. Derm., 1903, p. 292, showed a case (soc’y demonstration)
with lesions of “acnitis” of the face combined with lesions of “folliclis” on the elbows
and forearms; and the cases shown as folliclis at the Internat. Derm. Congress, at Ber
lin, 1904, that I saw certainly corresponded to what Prof. Duhring had described as the
small pustular scrofuloderm.
See also interesting report (“Folliclis of the Skin and Conjunctiva,” Jour. Cutan.
Dis., 1905, p. 337) of a case by Anthony, concerning which there had been several of
these various diagnoses made. See further an interesting review by C. J. White, “The
Modern Conception of Tuberculosis of the Skin,” Boston Med. and Surg. Jour., 1905,
vol. cliii, p. 291, especially the parts bearing upon “acnitis,” and “folliclis.”
ACNE VARIOLIFORMIS
IO57
usually slight in character; just as frequently, however, in my experience,
no positive suppuration is noticeable, the apex becoming crusted and
sinking down. Sometimes the summit is vesicular or vesicopustular.
In whatever manner the crust results, it is ordinarily quite adherent,
and after some days is detached, accidentally or spontaneously, and un
covers a somewhat puckered depression, red and often abraded looking;
this gradually heals, the redness lessens, and the process is at an end,
leaving on its site a pin-head to large pea-sized, usually rounded,
clean-cut, variola-like scar. The lesions vary considerably as to size
and to superficial or deep involvement. When matured they are from
small pea- to bean-sized, and in some cases are extremely superficial,
scarcely seeming more than crusted abrasions; in others they seem to
pervade the whole depth of the corium. They are often close together—
almost bunched in some instances, and in these latter the scarring is
quite disfiguring. Exceptionally they are grouped in a linear, circinate,
and even serpiginous manner. In other cases they are widely apart, and
scattered irregularly over the involved region. While often (and usually)
present in scanty or moderate numbers, they may be, exceptionally,
quite numerous. The course of the disease is essentially chronic, new
lesions appearing from time to time. Occasionally, after a variable period
of months, spontaneous cure takes place, but, as a rule, it is chronic and
persistent.
The favorite or classic sites are the forehead, just at the edge of the
hair, and the scalp. Other parts of the face, and especially the bearded
region, are not infrequently its seat, either alone or conjointly with the
scalp. The eruption is, however, in some instances found elsewhere, es
pecially about the trunk, anteriorly and posteriorly, and more particu
larly the upper part. It is also found upon the extremities, either in
dependently or conjointly with face or scalp involvement. In Pringle’s1
patient the disease began in the interscapular region, and only after
some time involved the face, and later still extended upward over the
scalp. I have had cases under observation in which the eruption was
found on face and upper extremities. In many cases there are no sub
jective symptoms, but in others there is considerable itching, and some
times sufficiently marked to be an annoying feature; this seems to be
present more frequently in the superficial cases.
Acne agminata type2 (acnitis type of Barthélemy) is usually limited
to the face and forehead, with a predominant tendency toward abun
dance and grouping on the brows, temples, cheeks below the orbits,
upper lip, and chin. The eruption, in addition to the parts named,
may also be exceptionally seen elsewhere (in Schamberg’s case and my
case there were some lesions on the wrists and hands, and several on the
penis). The eruption is indolent, and the lesions may undergo involu-
1 Pringle, Brit. Jour. Derm., 1900, p. 298 (case demonstration).
2 In this country this rare type has been reported by Trimble (Jour. Cutan. Dis.,
1908, p. 309, with case illustration), by myself (case presentation, Philadelphia Derm.
Soc’y Trans., ibid., p. 477), and by Schamberg, ibid., 1909, p. 14 (with case and histo-
logic illustrations, with review and references); Bowen, Jour. Cutan. Dis., 1910, p. 693
(case demonstration), reports a case of acnitis, associated with lesions suggestive of
lupus nodules and erythema induratum.
67
1058 DISEASES OF THE APPENDAGES
tion with or without suppuration, almost all leaving, as a rule, depressed
scars. After a time, usually months, the process may gradually dis
appear.
Etiology.—The malady is encountered in both sexes, and most
commonly between the ages of thirty and fifty, rarely under twenty.
Syphilis has been considered to be a factor in some instances, but this
I believe to be exceptional; most cases are observed in those entirely
free from this disease. Sabouraud1 believes the malady due to the
conjoint action of his microbacillus of seborrhea and staphylococci.
The latter were also found by Fordyce and by Touton; Fordyce was
inclined to consider them of etiologic importance; Touton, that they
may be simply accidental. It is not improbable, too, as Johnston and
a few others have stated, that in some of these cases, as well as in the
variously named allied or aberrant forms referred to, instead of a direct
microbic cause, the toxins of the organisms, among which are the toxins
of tubercle bacilli, may be also etiologic; this latter belief indicating a
relationship or a place among the tuberculids, and which is in accord
with my own views.
Pathology.—It seems probable that the eruption is the result
of microbic invasion. It is to be considered an inflammation of the
pilosebaceous structures, with ensuing destruction of the follicle and
surrounding derma, Sabouraud, as already intimated, believing that
it is a secondary infection upon a seborrheic basis. Fordyce is inclined
to the opinion that the more frequent occurrence among the poor, and
its appearance, primarily at least, in the majority of cases on the forehead,
which is exposed to pressure by unclean hatbands, would suggest the
probability of local infection. The pathologic histology has been studied
chiefly by Leloir and Vidal,2 Touton, Fordyce, Sabouraud. Their gross
findings are about alike, the principal difference being as to the depth
at which the lesion begins or involves, and this is probably owing to the
character, size, and age of the lesion examined. The lesions in Pick‘s3
case had no connection with the pilosebaceous follicle, and his findings
indicate that this is not always the starting-point. Fordyce found that
in the earliest stage the lesion had its seat in the superficial derma, in
this respect differing from the hidradenitis suppurativa which originates
in the subcutaneous tissue. The majority of lesions were perforated by
a hair. The earliest changes noted consisted of a dense round-cell infil
tration about the hair-follicles, generally above the situation of the se
baceous glands. In some of the sections Fordyce found the sebaceous
glands surrounded by the exudation, while in others they were quite
free. The sweat-glands were uninvolved, and, in fact, outside of the
inflammatory zone. The process extends laterally and upward, invading
the papillary and subpapillary areas. Cell disintegration and infiltration
of the outer root-sheaths occur, and all the layers of the follicle may share
in the destruction produced by the inflammatory process. Usually the
1 Sabouraud, “L’acné nécrotique,” Annales, 1899, p. 841 (with histologic and bac-
teriologic illustrations).
2 Leloir and Vidal, Traité descriptif des mal de la Peau, p. 23.
3 Pick, Archiv, 1889, p. 551.
ACNE VARIOLIFORMIS IO59
destructive action is limited to the upper half of the hair-follicle, the
lower part and the sebaceous gland remaining almost undisturbed. The
affected tissue is gradually separated en masse by a process of dry necrosis,
but less markedly so than observed in hidradenitis. The staphylococci
were found in the lymph-vessels and free in the tissues, and were espe
cially numerous about the middle and deeper portions of the hair-follicles
within the external and internal root-sheaths, in the connective tissue
about the sweat-glands, and in the subcutaneous connective tissue.
Diagnosis.—Acne varioliformis is to be distinguished chiefly
from a pustular syphilid and acne vulgaris. Its localization, in a large
number of cases, to the forehead and scalp is a differential point of value.
The sluggish, indolent character of the lesions, their slow course, and
the comparatively slight suppurative or necrotic action, with the result
ing varioliform scars, are more or less distinctive of all the types of
acne varioliformis. Its resemblance to a papulopustular syphiloderm is
sometimes striking, but the latter is almost always of wide distribution,
and is commonly associated with other symptoms of the disease. The
evident involvement of the sebaceous gland in acne, with the usually
preceding comedo formation, its localization on the face, its course, and
the absence of tendency, in most instances, to scar-formation, are points
of difference. Folliculitis decalvans can scarcely be confounded with it,
as this is only seen on hairy regions, commonly the scalp, leaves cicatricial
areas of alopecia, and with the periphery studded with minute inflam
matory sycosiform pustules—the characteristic lesions of the malady.
Prognosis and Treatment—As a rule, most cases finally yield
to remedial measures. It is prone to recur. Untreated, it persists,
sometimes indefinitely, although in other instances periods of quiescence
or entire disappearance are noted.
Treatment consists in the use of antiseptic applications, the most
valuable being 3 to 6 per cent, ointment of ammoniated mercury, lotions
or ointments of resorcin, 5 to 25 grains (0.35-1.65) to the ounce (32.),
and salicylic acid ointment of 3 to 5 per cent, strength. Fordyce found
an ointment containing sulphur and naphthol curative. The most
satisfactory treatment in my experience is a compound lotion of resorcin
in a saturated solution of boric acid for the non-hairy regions, and for
the hairy parts the resorcin lotion conjointly with the ammoniated mer
cury salve. The lotion is to be applied to the parts generally, and the
salve subsequently rubbed into the lesion. In view of a seborrheic basis
being a possible factor, as contended by Sabouraud, occasional remedial
application for this disorder after the acne is cured is advisable, as pos
sibly preventing a relapse. As to constitutional measures, these, if
called for, are to be based purely upon indications in the individual case.
Staphylococcic vaccine has been recently employed with alleged prompt
and favorable action.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |