| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
3. DISEASES OF THE SEBACEOUS GLANDS
SEBORRHEA
Synonyms.—Steatorrhea; Stearrhea; Acne sebacea; Ichthyosis sebacea; Fr., Acné
sebacée; Séborrhée; Ger., Schmeerfluss; Gneis.
Definition.—A functional disease of the fat-producing glands,
characterized by an excessive, and perhaps abnormal, secretion of fatty
matter, appearing on the skin as an oily coating, crusts, or scales.
Since the writings of Unna and others on dermatitis seborrhoica, which
have led to a withdrawal of many cases (see Dermatitis seborrhoica)
heretofore considered to be rightly placed under seborrhea, there is much
confusion as to exactly what conditions are to be properly included in
this disease. Oily seborrhea, of course, belongs here, and I believe also
all those cases of fatty crusted or scaly conditions which lack all signs
of inflammatory action. The division line is, however, an ill-defined one,
and there is a growing belief that all cases except those of oily seborrhea
show histologically evidences of inflammation.1
Symptoms.—Two varieties of seborrhea are usually found,
designated, according to whether there is practically only oiliness or
oiliness with scale or crust accumulation; the former is that known as
seborrhœa oleosa, and the latter, seborrhœa sicca. The qualifying term
“sicca,” or dry, in my judgment is in the present state of our knowledge
an improper one, as those cases in which the accumulation is truly dry—
not oily or fatty—are necessarily relegated to dermatitis seborrhoica.
The term, as here employed, will not refer therefore to such types, but
essentially to those in which there is marked or moderate oiliness, with
scale accumulation or crusting added, and in which there are no
inflammatory symptoms. Such cases, I believe, exist, although, com-
1 See “Dermatitis seborrhoica,” and also Jackson and McMurtry’s, article on
“Seborrhœa capitis,” Jour. Cutan. Dis., 1912, p. 608.
1022
DISEASES OF THE APPENDAGES
pared to those belonging to seborrheic dermatitis, in relatively moder
ate number.
Seborrhœa oleosa (known also as hyperidrosis oleosa (Unna, Brocq),
acné sebacée fluente, stearrhœa simplex, seborrhœa simplex, etc) is
observed upon the scalp and face, usually conjointly, although it may
be relatively extremely slight in some cases on one or the other of these
regions. On the scalp the hair and skin are noted to be. oily and greasy;
the oiliness may be slight or quite perceptible, and may involve the whole
region, or be mainly upon the vertex portion. The hair looks moist,
sometimes glistening, and is often slightly sticky, stringy, or with a tend
ency, in women, to form into uncouth-looking, slightly agglutinated
locks, or there is a tendency to bunching or massing together. The
skin is oily to the touch, pale, often leaden-looking, and sometimes with,
apparently at least, rather patulous gland-ducts. There are no inflam
matory symptoms, except in occasional cases, when there may be here
and there slight hyperemia, patchy in character. Itching is rarely com
plained of in the oily variety. If of long continuance, there is very often
a tendency to hair loss, and in some instances finally of a more or less
pronounced character.
On the face, the favorite site for the oiliness is the nose and its imme
diate neighborhood; not infrequently, however, the forehead is also in
volved, and occasionally other parts of the face. In fact, in all cases there
is, as a rule, a slight oiliness of these several regions, or the entire face,
but it may be conspicuously so only on one or two of the regions named.
The skin is shiny, glistening, and the gland-ducts often patulous, and the
whole face presents a pasty-looking, soiled aspect. Not infrequently the
nose is somewhat congested, and usually of a sluggish red tint. In
addition, in some patients, comedones and scattered acne lesions are to
be seen, and in occasional instances there is a disposition shown here
and there, more especially on the scalp, for the secretion to dry and cake,
forming thin scaliness of dirty-gray or brownish-gray color. If in women,
the malady seems to be often associated with a tendency to hypertri-
chosis.
Seborrhœa Sicca.—In infants it is at birth more or less general,
though variable in quantity, and constitutes the so-called vernix caseosa
(also ichthyosis sebacea). It is apt to remain caked on the scalp for some
months, and while it must be looked upon as physiologic, not infre
quently, from irritation produced by decomposition or from harsh at
tempts to remove it, an eczema may ensue. In children and adults its
usual site is the scalp (seborrhœa capitis). In this form, in addition to
more or less oiliness, the fatty secretion and the exfoliating epidermic
scales, and some possibly from the lining membranes of the gland-ducts,
tend to accumulate in an irregular, thin, or somewhat thick, soft, unctu
ous, waxy-looking, gray or brownish coating. There is usually a variable
amount of itching. The skin beneath the crusts is not hyperemic, but
of the usual color or somewhat paler than normal, with, in some cases, a
tendency here and there to slight redness and development into dermatitis
seborrhoica. The gland-ducts are often somewhat stuffed with semi-
solid fatty matter. The hair is greasy and oily, sometimes massed or
SEBORRHEA
1023
bunched, and practically in the same condition as noted in seborrhœa
oleosa. In the crusted seborrhea there is a more decided disposition to
falling of the hair and consequent alopecia. The disease varies in
degree. It may be slight, with a variable amount of oiliness, and small
fatty scale or crust specks or small filmy fragments, which are found on
the scalp, scattered through the hair, and sometimes falling upon the
shoulders. This latter illustrates one variety of the condition known as
dandruff—of the oily or greasy form, in contradistinction to the dry
variety, pityriasis capitis (one form of dermatitis seborrhoica).
A mild degree of crusted or scaly seborrhea is sometimes seen upon
the face, occasionally alone, but more commonly in conjunction with the
disease upon the scalp; its usual site is about the nose, and sometimes on
the bearded region. As a rule, most cases of a greasy, scaly nature about
these parts present a slightly or moderately inflammatory basis, and be
long to the domain of dermatitis seborrhoica. The surface is noted to be
oily, and variously coated with a pasty, dried, greasy film, or a thin,
cheesy coating, and, especially about the nose, sometimes with dippings
down into the glandular openings.
Rarely a similar, apparently noninflammatory, condition is noted
on the chest, usually over the sternum and between the scapulae, and
is generally of irregular patchy or circinate formation, with projections
into the follicles. As a rule, however, an inflammatory element is added
in these cases, and the picture is then that of dermatitis seborrhoica.
Crusted seborrhea is also sometimes seen upon the glans and corona
of the penis, beneath the prepuce, where the secretion is usually relatively
active, and, if permitted to collect, forms a flaky, irregular, thin, cheesy
coating which undergoes decomposition, and causes more or less irrita
tion or a positive balanitis. The same condition may arise in women,
about the clitoris and vulvar folds, unless the parts are frequently
cleansed, and a vulvitis results. Occasionally the pubic region, like the
scalp and other hairy parts, is the seat of a flaky or thin greasy coating,
conjointly with oiliness.
Etiology.—Exclusive of the seborrheic condition in the new-
born and early infantile life, the malady is most frequent between the
ages of fifteen and thirty, when the glandular structures are usually most
active, although it is not uncommon, especially in women, toward the
climacteric. It is met with in both sexes, and with, upon the whole,
but little preponderance either one way or the other. Those of dark
hair and complexion are the usual subjects for the oily variety. General
debility, anemia, chlorosis, dyspepsia, and similar disorders are to be
variously looked upon as contributory, if not causative. The disease
is also noted to develop after severe constitutional diseases, especially
after the various exanthemata. Scrofulosis must also be considered as
furnishing a good basis for its production. Seborrhea of the nose is
apparently due in some cases to intranasal pressure or obstruction (Seiler,
Besnier, Doyon, and others). In some instances, it is true, the disease
seems to be due to a loss of tone in the glands and skin, and to be entirely
independent of any constitutional or predisposing condition. The view
advanced in recent years, that the disease is of parasitic nature and con
1024
DISEASES OF THE APPENDAGES
tagious (Unna, Sabouraud, and others), has been steadily gaining ground,
and its occurrence in several or more members in certain families bears
as much upon the question of contagiousness as it does upon hereditary
or family tendency.
Pathology.—Seborrhea, as observed in the types just described,
is to be considered as a disease chiefly and probably wholly of the
sebaceous glands, and functional in character. Unna and Meissner
would have us believe that the coil-glands (sweat-glands) secrete the
oil, and that (Unna) the seba
ceous glands are not involved
in this malady, except secon
darily. Unna, therefore, sug
gests for the oily form the
name hyperidrosis oleosa, but
Beatty’s1 investigations go to
show that at least in the oily
form and the vernix caseosa
the secretion is not a product of
the sweat-glands. While it is,
I believe, true that secretion
from the sweat-glands does
contain oil at times, at least,
nevertheless, one needs but ex
amine a case of seborrhea of
the types here defined and the
exit from the sebaceous gland-
ducts of fatty secretion is at
once evident. Moreover, its
favorite situations are those
where the sebaceous glands are
most numerous and most
highly developed. Sabouraud2
does not state it too strongly
when he says that seborrhea
has two essential symptoms—
an overproduction of normal
sebum and a dilatation of the
sebaceous gland-duct openings.
The oily secretion and the fatty collection found in the gland-ducts
and also that upon the surface are chiefly composed of fatty matter,
although Elliot3 found that the plugs in the ducts were composed of
epidermic cells, derived from the epidermic lining of the follicular open
ing, impregnated with fatty hypersecretion. Van Harlingen,4 who made
some careful investigations, concludes that: “(1) The sebaceous secretion
1 Beatty, “Seborrhea,” Brit. Jour. Derm., 1894, p. 161; also “The Functions of
the Glands of the Skin,” ibid., 1893, p. 97 (both valuable contributions).
2 Sabouraud, Annales de l` lnstitut Pasteur, 1897, p. 134; and Annales, 1897,
P. 257.
3 Elliot, Morrow’s System,, vol. iii (Dermatology), p. 789.
4 Van Harlingen, “The Pathology of Seborrhea “ Arch. Derm., 1878, p. 97.
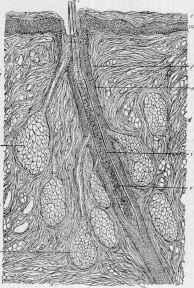
Fig. 256.—Vertical section through the
scalp of a newborn child suffering from sebor-
rhœa neonatorum (X 250): e, Corneous layer;
m, rete mucosum; s, shaft of hair; r, root of
hair, cut obliquely; i, inner root-sheath; 0,
outer root-sheath; f, hair-follicle; g, g, en
larged sebaceous glands, with ducts; d, d,
corium; v, veins in the corium (courtesy of
Dr. L. Heitzmann).
SEBORRHEA
1025
is derived from fatty metamorphosis of the enchyma cells of the sebaceous
glands. These cells are homologous with those of the stratum mucosum
of the skin. They have nothing in common with the cells of the horny
layer. (2) Seborrhea is a disease of the sebaceous glands, characterized
by the pouring out of an increased quantity of sebum, more or less altered
in chemical and physical composition. In comedo and seborrhœa sicca,
properly so called, the secretion is condensed to a fatty consistency,
while in seborrhœa oleosa it remains in an oily state. In each of these
affections, however, microscopic examination shows epithelial cells in a
state of more or less complete fatty degeneration, and breaking down
into granular débris. Horny cells are found only adventitiously.”
Sabouraud believes that seborrhea is due to a short microbacillus.1
It is always to be found in the upper part of the hair-follicle, and a sebor-
rheic cocoon which develops, containing the bacillary colony, by inter
fering with the function of the hair-papillæ, gives rise to the secondary
hair loss and sometimes permanent alopecia. Further evidence is, how
ever, needed before Sabouraud’s conclusions can be admitted. Scham-
berg2 found this bacillus in individuals who presented no trace of sebor-
rhea. As the observations of Unna, Sabouraud, Brooke,3 and others
show, the seborrheic process often has an influence in materially influ
encing other cutaneous eruptions, notably eczema, acne, acne rosacea,
syphilis, psoriasis, etc
Diagnosis.—Oily seborrhea can scarcely be mistaken for any
other disease; the oily, greasy character and appearances and the region
involved are sufficiently distinctive. The crusted, scaly form is to be
differentiated from eczema, dermatitis seborrhoica, psoriasis, and possibly
ringworm. The rather diffused character of seborrhea, the greasy, oily
nature of the scaliness or crusts, the absence of all inflammatory symp
toms, the usually dilated gland-ducts, containing sebaceous matter, are
points of difference from those of the several diseases named; moreover, in
these latter there are noted, except in eczema, rather sharp definition to
the areas and inflammatory action. In eczema the inflammatory char
acter is sufficient to prevent error. It is true, however, that the step
from seborrhea to dermatitis seborrhoica is often a short one.
Prognosis and Treatment.—The. prognosis of seborrhea is
favorable, although it must be said that the disorder is sometimes
obstinate, and that there is a strong disposition to recurrence. In
moderately severe and in severe cases of seborrhea of the scalp, of pro-
1 Tiéche, Archiv, 1908, vol. xcii, p. 125 (with brief review and some references), has
made some investigation as to the micro-organisms of the scalp, taking tissue from the
scalps of dead bodies as soon after death as possible. He found the Malassez spores in
48 cases—96 per cent.; in 44 per cent, seborrhea bacilli were present in numbers, ab
normal forms in 20 per cent.; hyphæ and spores, having considerable resemblance to
microsporon furfur, were found in 10 cachectic subjects. A table showing the relation
ship of bacterial and fungous growths to soil (subjects) is added.
2 Schamberg, “Remarks on the Microbacillus of Seborrhea,” Jour. Cutan. Dis.,
1902, p. 99.
3 Brooke, “The Relations of the Seborrheic Processes to Some Other Affections of
the Skin,” Brit. Jour. Derm., 1889, p. 247; see also literature reference to Sabouraud’s
papers in connection with acne; also paper by W. Anderson, “On Seborrhea and its
Results,” ibid., 1900, p. 276; and by R. W. Taylor, “The Seborrheic Process and the
Early Syphilitic Eruptions,” Jour. Cutan. Dis., 1890, p. 161 (with 2 good cuts).
65
1026
DISEASES OF THE APPENDAGES
tracted duration, loss of hair is not an unusual sequence, although in
most cases, if not too long neglected, a regrowth may be looked for.
In some instances of seborrhea local treatment alone is required;
in most cases, however, the general condition is below the normal stand
ard; constitutional remedies are to be administered according to indica
tions. Chlorosis, anemia, and digestive disturbances certainly seem to
have a strong predisposing influence, if not directly causative; and a
removal of any of these several conditions will often have a favorable
action upon the disease, or make it more promptly responsive to suitable
local measures. Iron, strychnin, quinin, cod-liver oil, digestives, and
laxatives are, therefore, to be prescribed according to the indications
in the individual case. Arsenic may be tried in rebellious cases; and
ichthyol (the ammonio-sulphate), in doses of 5 to 15 grains (0.3-1.)
three times daily, is highly praised by Elliot for the oily variety. A
vaccine1 made from the microbacillus might be tried in obstinate cases.
In instances in which the disease is practically limited to the nose, the
possibility of intranasal pressure or obstruction should be eliminated, or,
if present, appropriate treatment recommended.
In the management of seborrhea frequent washing with soap and
water is usually necessary, in order that the parts can be kept free from
the oiliness or crusting, and for this purpose a mild toilet soap can be
used, or in those of sluggish, non-irritable skin the tincture of green soap.
In obstinate scalp cases to the latter can be added 10 to 30 grains (0.65-2.)
of resorcin to the ounce (32.). The frequency of the washing depends
upon the severity of the disease and the character of the remedies em
ployed; if the oil or fatty accumulation is rapid, once every two or three
days would be required for the scalp and once daily for the face. In
fact, the face requires such washing as a routine measure once daily, and
preferably at bedtime and before the application of the selected remedy.
When salves are employed, a certain amount of added messiness results,
especially upon the scalp, and cleansing becomes more frequently neces
sary. After the disease becomes less active the scalp can be washed
every three to ten days; as a rule, however, frequent shampooing, con
joined with remedial applications once or twice daily, is often necessary
in the scalp cases, especially those of the markedly oily variety. As the
condition improves treatment can be less frequent and gradually inter
mitted, or applications made at intervals of several days. In the removal
of the greasy collection in infants care is to be taken that the skin be not
irritated, for it is an easy matter in these cases to start up eczema; strong
soaps should not be used, and if the crusting is adherent, as it often is on
the scalp, it can be softened by oil applications, or, if persistent, with
starch poultices.
The chief remedies to be employed in the external treatment of
seborrhea are resorcin, sulphur, ammoniated mercury, salicylic acid,
and boric acid. Resorcin is the most valuable, and is prescribed more
frequently and satisfactorily as a lotion, 1 to 10 per cent, strength,
1 Savill, Practitioner, March, 1911, p. 392, reports a cure of a chronic case of sebor-
rhœa oleosa of the scalp with vaccine made from the culture of the microbacillus of
Sabouraud.
SEBORRHEA 1027
made up with 1 part alcohol and 3 to 6 parts water, or in some cases,
especially on the scalp, the pure alcoholic solution seems best. If too
drying, glycerin can be added to the aqueous lotion, and castor oil to the
alcoholic one—a few minims to the ounce (32.). In those of very light
or gray hair, if used, it should be carefully and in scanty quantity; if
used freely, the hair becomes wet with it and there often results a dirty
or dingy-looking staining. Resorcin may also be used in ointment form,
made up with vaselin or cold cream, of about the proportion of 20 to 60
grains (1.3-4.) to the ounce (32.). Both as a lotion and ointment the
weaker strength should be tried first, and then the proportion increased
—for occasionally this drug is found to act as an irritant. Sulphur is
applied in but one form to the disease as it occurs upon the scalp—as
an ointment, from ½ to 2 drams (2.-8.) of precipitated sulphur to the
ounce (32.) of petrolatum or benzoated lard. Ammoniated mercury, in
a strength of from 20 to 60 grains (1.3-4.) to the ounce (32.) of ointment,
is likewise a valuable application—upon the whole probably less generally
useful than the sulphur ointment, but colorless and more elegant. Sali
cylic acid may also be employed alone in the form of an ointment, from
10 to 30 grains (0.65-2.) to the ounce (32.), but it is more frequently
employed with sulphur or ammoniated mercury in compound ointments.
As a rule, the lotions are much more efficacious for the oily form
than are ointments, and probably also in the crusted variety, but in
the latter, when scale accumulation is at all rapid, ointments are often
demanded, and, indeed, in some instances, act more satisfactorily. A
good plan in these cases is to use a lotion up to within a day or two of the
time for shampooing, and then to employ a pomade, resuming the lotion
after the shampoo. Upon the whole, petrolatum is a good base for the
scalp, and often somewhat improved by 1 or 2 drams (4.-8.) of cacao-
butter to the ounce (32.); for the face, cold cream can take the place of
the petrolatum. Davis commends highly a “stearoglycerid ointment"
as the ointment base,1 as not being greasy and readily washed off. In
addition to the lotions already named which may be used for the disease
upon the face, the sulphur lotions employed in acne are also of service
in some instances; they are to be tried in weak proportion at first, as this
remedy sometimes irritates in these cases. Carbolic acid as a lotion is
also useful in seborrhea of the scalp, but has the disadvantage of odor;
it can be prescribed in 1 to 3 per cent, strength, preferably in alcohol,
and to which, if found too drying, a few minims of castor oil can be
added. A lotion of corrosive sublimate is also sometimes of service,
both for scalp and face cases, and of either variety; it may be used in
the strength of 1 or 2 parts to 1000, and either alone or with the resorcin
lotion as a base.
In the treatment of the disease about the glans penis and vulva
frequent ablutions—twice daily at least—should be enjoined. The
milder lotions of boric acid and resorcin have special application on
these parts. Also weak lotions of zinc sulphate and tannic acid; of the
former, 1 to 3 or more grains (0.065-0.2) to the ounce (32.), or of the latter,
a saturated solution. A compound lotion, using the boric acid solution
1 See treatment of Alopecia for formula.
1028 DISEASES OF THE APPENDAGES
as a basis, with the zinc sulphate added, and if there are any abrasions,
with the addition of 10 or 15 grains (0.65-1.) of finely powdered zinc
oxid or bismuth subnitrate to the ounce (32.), often acts satisfactorily.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |