| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
MILIARIA
Synonyms.—Lichen tropicus; Heat-rash; Prickly heat; Red gum; Strophulus; Fr.,
Miliare; Ger., Schweissflechte.
Definition.—An acute, mildly inflammatory disorder of the
sweat-glands, characterized by numerous pinpoint to pin-head-sized,
discrete but closely crowded papules, vesicopapules, and vesicles, or an
admixture of these several lesions, and accompanied by more or less
pricking, burning, or itching.
Symptoms.—There are two clinical varieties of this affection,
one composed wholly or almost entirely of papular lesions, and the other
of vesicular lesions. In the majority of cases, however, while there
is a preponderance of one type of lesion there is a distinct admixture
of the two. Some lesions, too, are neither pure papules or pure vesicles,
but midway between these—vesicopapules. It is especially to the
papular type—miliaria papulosa—that the names lichen tropicus and
prickly heat are given, although these terms, more especially the latter,
are often used synonymously with the disease name miliaria, whatever
may be the type. It makes its appearance suddenly, occurring upon a
limited portion of the body, or, as commonly observed, involving a greater
part of the entire integument. The lesions are minute, for the most
part pin-head-sized, and rarely exceed the size of millet-seeds. In color
they are pinkish or bright red, and closely crowded, although they re
main discrete, so that the entire region affected is more or less uniformly
hyperemic While in this type the whole eruption may be entirely
made up of papules, it is usual to see an intermingling of vesicopapules
and vesicles.
The vesicular variety—miliaria vesiculosa—is that variety of miliaria
in which the eruption is distinctly vesicular. The lesions are small—
for the most part the size of pinpoints or pin-heads. They are present
in great numbers, are acuminate or conic in shape, never tend to coal
esce, and show no disposition to rupture. The lesions have a slight pink
ish or red areola, and being so closely crowded, this gives the whole field
of eruption its red and inflammatory aspect—miliaria rubra. Later
the areolæ fade, the transparent contents of the vesicles become some
what opaque and yellowish-white, and the eruption has a whitish or
MILIARIA
IO89
yellowish cast—miliaria alba. Occasionally the contents of some become
seropurulent or even purulent.
In all cases of miliaria there is usually a feeling of burning, prick
ing, or itching, which may be slight, moderate, or intense in character.
Sweating generally is noted to precede and accompany the eruption.
The lesions tend to disappear in the course of some days or one or two
weeks, the papules gradually fading away; the vesicles disappear by
absorption or desiccation, the epidermal covering, which is always ex
tremely thin, disappearing by slight, at times scarcely perceptible,
desquamation. When the closely crowded vesicular lesions are broken
open by rubbing or accidentally, the liberated contents, minute in quan
tity, dry to insignificant thin crusting. In cases in which the cause
continues there are fresh outcroppings, and the disease is thus prolonged,
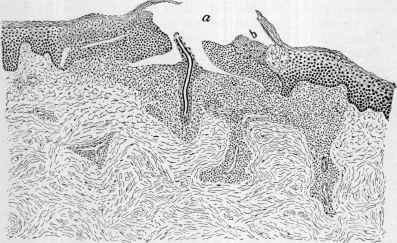
Fig. 269.—Miliaria, vesicopapule. showing vesicle (a) with the excretory sweat-duct
in the lower central part, and inflammatory changes in the rete (b), and also in the
upper part of the corium and deeper down along the blood-vessels (courtesy of Dr. A.
R. Robinson).
or in such instances it may be transformed into a veritable eczema,
although such termination is not common. Not infrequently in these
prolonged cases, and more especially in infants and young children,
boils and small cutaneous abscesses are seen in association with it.
Etiology and Pathology.—Extreme heat is the essential causa
tive factor; this may be due to the weather temperature or to working
in an overheated room, from vapor baths, or from being overclad. Those
who perspire freely are its most common subjects, more particularly
infants and young children, and middle-aged adults who are overfleshy.
In the latter free drinking of beer or other alcoholic drinks is sometimes
a factor. In some instances debility seems to be of predisposing in
fluence.
The affection is due to sweat obstruction, with mildly inflammatory
symptoms as a cause or consequence; with congestion and exudation,
69
1090
DISEASES OF THE APPENDAGES
with, at times, sweat effusion about the ducts, leading to the formation,
according to the intensity of the process, of papules or vesicles. But
there is still some difference of opinion, however, as shown in the follow
ing briefly stated views: (1) that it is an inflammatory disease of the
epidermis and not an affection of the sweat-glands alone; the lesion
occurring around a sweat-duct in the rete and upper part of the corium,
with slight inflammatory effusion and usually transudation or retention
of sweat, the vesicular lesions all being connected with the sweat-glands
(Robinson);1 (2) that the vesicles are due to dilated sweat-ducts, the
papules to the occurrence of cysts filled with cellular elements, and of
cysts in the lower region of the rete, and to circumscribed swelling in the
immediate neighborhood of a sweat-pore (Pollitzer2); (3) that no con
nection between the sweat-gland and vesicle can be found, and that the
lesions are purely of inflammatory origin, or eczematous, probably due
to irritation produced by the sweat on the surface (Török3). As all are
good observers, it is probable that the lesions vary somewhat in origin
and formation.
Diagnosis.—The rapidity of the outbreak, the closely crowded
lesions, the mild inflammatory aspect, the preceding and often accom
panying sweating, absence of tendency in the vesicles to spontaneous
rupture, the external high temperature factor, and absence of consti
tutional symptoms, are usually sufficiently distinctive. Papular eczema
is in most cases rather limited in extent, the lesions are larger and mark
edly inflammatory, come out more slowly and are persistent, and, where
close together, there is a good deal of inflammatory swelling and infiltra
tion. The same features serve to distinguish vesicular eczema; moreover,
in this latter there is distinct tendency to spontaneous rupture of the
lesions and characteristic gummy oozing and crusting. There is a re
semblance to sudamen, but in this latter there are no inflammatory signs,
the vesicles being transparent, whitish, resembling minute dewdrops,
and seen in association with some febrile or cachectic state. Miliaria
or similar lesions occur sometimes in the exanthemata, but the consti
tutional symptoms and the accompanying or quickly following charac
teristic eruption of the latter serve as differential points.
Prognosis and Treatment.—Under favorable conditions at the
end of several days or a week or two the disease has come to an end.
In some cases the cause persisting, there may be rapidly recurrent at
tacks, so that the eruption may almost be continuous over several weeks
or longer, with or without occasional furuncles, or eventually developing,
especially in the folds, into an intertrigo or an eczema.
In the management of the affection its common cause—excessive
heat from high temperature or from too much clothing—should be kept
in mind. The disorder is thought to be more frequent in those of de
bilitated constitution, and for this reason treatment of a tonic character
is sometimes appropriate. In those of full habit and stout, refrigerant
1 Robinson, Jour. Cutan. Dis., 1884, p. 362, and in Bangs-Hardaway’s Amer. Text
book, p. 1096.
2 Pollitzer, Jour. Cutan. Dis., 1893, p. 50 (with several cuts), and New York Med.
Jour., 1894, vol. lix, p. 12.
3 Török, abs. in Monatshefte, 1891, vol. xiii, p. 437.
MILIARIA 1091
and acid drinks are apparently of service. Saline laxatives should be
administered in the beginning, and repeated from time to time in the
more persistent cases.
As a rule, however, removal or modification of the cause, and the
application of a dusting-powder or cooling and astringent lotions are
all that are required in the average case. The dusting-powder may con
sist of zinc oxid, boric acid, talc, and starch, singly or of equal parts.
The simple household remedy of one part vinegar or alcohol to several
parts water will also often be sufficient in such instances. In rather
extensive cases, in which itching or burning is a prominent symptom,
the following lotion may be prescribed:
R. Ac carbolic, 3ss (2.);
Ac boric, 3ij (8.);
Alcoholis, f3j (32.);
Aquæ, q. s. ad Oss (256.).
Or one of thymol, 5 to 10 grains (0.35-0.7), sodium borate, 8 grains
(0.55), alcohol, 1 ounce (32.), and water enough to make ½ pint (256.),
may be employed. In infants or others in whom there is a distinct
tendency to furuncular complication, a plain saturated solution of boric
acid, with 1 or 2 grains (0.065-0.13) of resorcin to the ounce (32.), is
especially to be commended. In some instances one of these lotions,
followed immediately by a dusting-powder, is more grateful. In those
persons of rather stout condition, who are frequently subject to the affec
tion, and who perspire somewhat freely, the daily use of a dusting-
powder of 1 part salicylic acid to 30 to 50 parts boric acid will, if the pa
tient avoid active exercise and overclothing, often prove a preventive.
Miliary fever1 (sweating sickness; miliary sweat rash; sudor anglicus;
English sickness; Fr., suette miliare) is an epidemic disease of rare and
scarcely known occurrence in recent years, in which profuse sweating
and miliaria are conspicuous symptoms. The last epidemic occurred in
France. The earliest symptoms are ill-defined prodromata, such as
feverishness, weakness of the legs, and general malaise and nervous
symptoms, the last consisting of feelings of epigastric constriction, of
suffocation, sometimes paroxysmal, and agitation, delirium, etc., and
accompanied by copious sweating. Cramps and constriction of the
muscles are also observed. The tongue is coated and the bowels con
stipated, and in the early stage cough is habitual and epistaxis generally
abundant. The eruption soon presents, characterized by two chief
features: first, a miliary papule, transformed later into a vesicle, and,
second, a polymorphous erythema. This latter is of three forms—
a morbilliform eruption, a scarlatinoid rash, and purpura. The morbil-
liform rash first presents, followed by the scarlatinal and purpuric char
acters. In some instances the eruption remains morbilliform, and in
some cases the earliest rash is the scarlatinal.
The eruption appears first on the face, and then spreads to the
1 This description is abbreviated from an editorial review, Lancet, Oct. 1, 1887, p.
671, of Brouardel’s report of “L’epidemie de suette miliare du Poiton,” Bull. Acad. Med.,
1887.
1092
DISEASES OF THE APPENDAGES
neck, trunk, and upper limbs, and finally to the legs—the last often
being much less involved than the other parts. The veil of the palate
is often dotted over with red spots. The eruption frequently shows itself
in two or three successive crops, the previous crop disappearing com
pletely and rapidly, to be followed by another. The purpuric spots,
however, are apt to remain a long time. As soon as the eruptive stage
is pronounced, the general symptoms gradually abate. The so-called
“suette blanche" variety is composed of papules, which remain hard and
opaque, with but little, if any, tendency to vesicular transformation.
The final disappearance of the eruption is followed by desquamation.
The malady is fraught with danger, the mortality varying from 12 to 33
per cent.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |