| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
FRAMBESIA2
Synonyms.—Yaws; Frambœsia tropica; Pian; Bouba; Polypapilloma tropicum;
Tonga; Amboyna button; Parangi; Fr., Pian; Ger., Beerschwamm.
Definition.—An endemic, highly contagious disease with or
without constitutional disturbances, characterized primarily by an
eruption of papules which develop into more or less exuding raspberry
or cauliflower-like nodules or patches.
1 Row, Brit. Med. Jour., March, 9, 1912, p. 540, states that rapid healing in three
cases seemed to result from vaccine treatment—vaccine being made from cultures from
an experimental lesion in a monkey.
2 Literature: J. Numa Rat, Yaws: Its Nature and Treatment, London, 1891 (with
bibliography to 1887); review and résumé of the same by Malcolm Morris, in Brit.
Jour. Derm., 1892, p. 63; Beaven Rake, “Postmortem Appearances in Cases of Yaws,”
ibid., 1892, p. 371; Breda, “Beitrag zum klinischen und bacteriologischen Studium der
brasilianischen Frambœsia oder Boubas,” Archiv, 1895, vol. xxxiii, p. 3 (2 colored plates
of the disease, and 2 plates with histologic cuts; unsuccessful experimental animal
inoculations; literature references); Pierez, “Frambcesia,” Trans. First Pan-American
Med. Cong., Washington, 1895, part ii, p. 1764 (an elaborate paper); Daniels, “The
Non-Identity of Yaw and Syphilis,” Brit. Jour. Derm., 1896, p. 426; Powell, “Yaws
in India,” ibid., p. 457 (a clear presentation of the subject in all its aspects); Hirsch,
Handbook of Geographic and Historic Pathology, Syd. Soc ed., vol. ii, p. no (with
bibliography); Dyer’s paper in Morrow’s System, vol. iii. (Dermatology), p. 687, gives
a good account with bibliography; Scheube, Die Krankheiten der warmen Länder,
2d edit., 1900; Kynsey, Brit. Med. Jour., 1901, ii, p. 802 (differentiation from syphilis).
Nicholls, Gov't Rep. on Yaws in West Indies, 1894 (with colored illustrations), condensed
critical report of this by Wallbridge and Daniels, in New Sydenham Soc’y vol. for
1897; Manson’s Tropical Diseases, 3d edit., 1903; Dalziel, Jour. Trop. Med., 1904, p.
288 (occurrence and probable origin in South China); R. Koch, Archiv, 1902, vol. lix,
p. 5 (with case illustrations); J. Numa Rat, Jour. Trop. Med. 1904, p. 86 (its introduc
tion in Auguilla in 1902), and Select Colonial Med. Reports, 1904, p. 177, and Jour. Trop.
Med. 1904, p. 317 (alkaline treatment); Modder, ibid., p. 213 (bacteriology and alkaline
treatment); Dalziel, ibid., p. 288 (in South China); Pernet, ibid., 1905, p. 262 (De
Rochas’ views, and histologic note); Woolley, Amer. Med. 1904, vol. viii, p. 242;
Graham, Brit. Med. Jour., 1905, ii, p. 1275; Jeanselme, ibid., p. 1276, and La Pratique
Dermatologique, vol. iii, p. 868 (in French Indo-China); De Boissere, Jour. Trop.
Med., 1904, p. 179 (tertiary manifestations); Henggeler, Monatshefte, 1905, vol. xl, p.
235 (a comprehensive paper, with 6 case illustrations, a good review and bibliography
Wellman, Jour. Trop. Med., 1905, p. 345 (spirochætæ findings); Castellani, Brit.
Med. Jour., 1905, ii, p. 1330 (spirochætæ findings and also oval chromatin-containing
bodies), and also in ibid., pp. 1280, 1330, and 1438; and Jour. Trop. Med., 1906, p. 1
(differentiation from syphilis); Macleod, ibid., ii, p. 1266; McCarthy, Indian Med.
Gaz., 1906, p. 53 (in lower Chindivin District, Upper Burma); Gimlette, Jour. Trop.
Med., 1906, pp. 149, 175, and 186 (The Pura of the Malay Peninsula); Neisser, Baer-
mann, and Halberstaedter, Münch, med. Wochenschr., July 10, 1906 (experimental
inoculation in apes); Breda, Giorn. ital., 1906, p. 98; Castellani, “Frambœsia Tropica,”
Jour. Cutan. Dis., 1908, p. 151, gives an admirable exposition and review, with 14
excellent illustrations; Howard, “Tertiary Yaws,” Jour. Trop. Med., July 1, 1908, p.
197 (observations based upon nine years’ residence in central Africa, in the country
bordering on the southern half of Lake Nyassa); Ashburn and Craig, “Observations
upon Treponema Pertenuis (Castellani) of Yaws and the Experimental Production
of the Disease in Monkeys,” Philippine Jour, of Sci., Oct., 1907, p. 441 (with excellent
photomicrograph and extensive bibliography); “Contribuicao ao Estudo da Bouba,”
by O. Silia Aranjo, Rio de Janeiro, Rodriques Co., 1911; C. J. White and E. E.
Tyzzer, “A Case of Frambœsia,” Jour. Cutan. Dis., March, 1911, p. 138 (patient,
Porto Rican sailor, lesions with somewhat horny verrucous covering; spirochætæ found
corresponding to Castellani’s spirochæta pertenuis; reproduction of disease in a monkey;
case, spirochætæ, and histologic cuts).
FRAMBESIA 851
Symptoms.—There is usually a prodromic stage, or stage of
incubation, dating from the time of inoculation to that of the appear
ance of the inoculation lesion. While during this period such symptoms
as malaise, slight fever, anorexia, hyperidrosis, vertigo, and rheumatic
pains, etc, with pallor of the skin, may be present and even quite pro
nounced, especially in young children, they are often wholly wanting.
At this time or somewhat later, but as a rule before the papular eruption
develops, furfuraceous whitish, usually pruriginous patches appear on
the trunk and limbs; these may coalesce and cover large portions of the
body. Some of these desquamating patches may disappear early, and
leave the skin lusterless and rough; others may remain, and sometimes
new ones appear, throughout the whole course of the disease (Castellani).
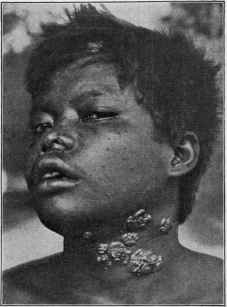
Fig. 205.—Frambesia (courtesy of Dr. O. Henggeler).
It is upon these patches that many writers state the elements of the erup
tion appear. On the other hand, Henggeler has not observed these
prodromal changes in the skin at all. The period of incubation varies
much, from ten days to several weeks or longer;1 and is followed by the
so-called primary stage, characterized by the development of a papule
at the point of inoculation. This appears as a hard papule, usually
itchy in character, which gradually enlarges and presents upon its sum
mit a depressed yellow spot of inspissated secretion; this latter tends to
spread until the whole papule is absorbed by the ulceration and crusted
over (MacCarthy); it quite frequently becomes rapidly papillomatous.
Instead of a papule the beginning lesion may be a pustule (Henggeler).
1 In the experiments by Neisser, Baermann, and Halberstaedter (loc. cit.) upon apes
the period of incubation varies from thirteen to ninety-six days.
852
NEW GROWTHS
The primary lesion is generally extragenital, and may occur on any part,
probably most commonly on the extremities in adults and on the hands
and face in children; and in infants who contract it from an affected
mother, in the corners of the mouth—the breast in women being a not
uncommon site. The inoculation lesion, or beginning lesion, may also
present and continue as a nodule or tubercle, desquamating and disap
pearing by absorption; also as a kerion-like formation; and sometimes
as a papillomatous growth, similar to the typical lesion of yaws, to which
the name of “mother yaw” is sometimes given. It is quite variable in
size, from a fourth to an inch or more in diameter. Some observers
have, however, doubted the existence of an inoculation lesion, looking
upon this so-called formation as simply a part or an early lesion of the
general eruption.
With care and treatment this initial or primary lesion is commonly
of but a few weeks’ duration; but if uncared for may, especially if it
had developed into an ulcer, last for several months. Following this
or during its development, and sometimes almost synchronously with
its first appearance the papular eruption of yaws is noted—the so-called
secondary stage of the disease. This consists of a variable number
(sometimes scanty, but usually numerous) of papules or tubercles of
but little more than millet-seed size, and commonly appearing, primarily
at least, on the favorite localities—the face, especially about the lips, the
neck, arms, and genitalia; and being, as a rule, least abundant on the
trunk. It may be limited and regional; on the other hand, it may be
extensive and general, and when so, and especially if occurring late,
it indicates a protracted attack (Manson). The advent of this eruptive
stage is quite frequently signalized by a recrudescence of the systemic
symptoms, but which subside, or measurably so, when the eruption is
well out. Pains in the limbs, sometimes quite severe, may persist for
some time (Henggeler). The lesions, while small at first, soon grow rap
idly larger, are usually conic in shape, the summits becoming yellowish
in color, and often exhibiting a central depression, so that some at this
time may suggest a rough resemblance to beginning variola pustules
(R. Koch). From these papules the typical eruption of yaws develops;
for along with the development of this yellowish summit the lesions
become somewhat broader based, some of them much larger, and crust
over. Many may, however, disappear, some before and some after this
stage is reached. On removing the crust, which may fall off sponta
neously, the surface is noted to be papillomatous, with a raspberry aspect,
and discharging an offensive, dark yellow, acid fluid. Rat says the
appearance is much less like a raspberry than it is like the top of a pickled
cauliflower. Several or more of these lesions may coalesce and form large
areas of similar character, crusting and discharging; and this tendency
to coalescence, according to de Rochas, is much more common or more
pronounced in children than in adults. In some cases fissuring is to be
noted in some of the nodules and patches. After a time the lesions gradu
ally flatten down, change to a yellowish or whitish color, and eventually
disappear, leaving a spot characterized in negroes by increased, and in
the white by lessened, pigment. The larger lesions and confluent areas
FRAMBESIA 853
sometimes break down and ulcerate, finally healing and leaving scars.
Some of the confluent groups may tend to clear up centrally, and a patch
is then seen with a ring-like edge (ringworm yaws). In some of the
patches a process of hyperkeratosis sets in; they become of much harder
consistency, and, especially those on the feet, may be covered with
numerous hard, verruca-like, small protuberances.
The disease may, after thus lasting for several weeks to several months,
gradually come to an end, favorable changes taking place and recovery
ensuing. In others there are fresh outcroppings from time to time of
the papular eruption, with not infrequently a recrudescence of the sys
temic symptoms, and with the development of some or all of the new
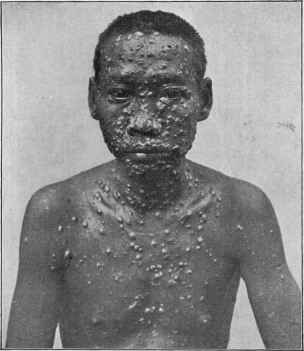
Fig. 206.—Frambesia (courtesy of Dr. O. Henggeler).
papules into the characteristic “yaws.” Occasionally some of these
latter break down into ulcers. It is, therefore, not uncommon to see
all varieties of lesions in the same case: furfuraceous patches, variously
sized papules, variously sized “yaws,” and in extreme and broken-down
cases sometimes a few or many ulcers as well. Distinct glandular en
largement has been noted by some observers and not noted or denied
by others. The mucous surfaces are hardly ever affected, unless about
the lips, around the angles of the mouth, and in the nostrils, where the
yaws often form clusters (Manson).
In chronic cases, especially in broken-down adults, the “yaws,”
more particularly the confluent areas, may undergo disintegration and
854
NEW GROWTHS
destructive ulcerations, bearing some resemblance to the gummatous
ulcerations of syphilis; and some of these may persist long after the
general and ordinary lesions have disappeared; furnishing in some in
stances doubtless cases of so-called “endemic ulcers,” and “tropical
ulcers.’’
There is much difference of opinion as to a tertiary stage of yaws,
with lesions and symptoms akin or somewhat akin to those noted in
tertiary syphilis; most observers deny its occurrence and claim in such
instances that there has been either a mistake in diagnosis or that there
has been a coincident or subsequent syphilitic infection; nevertheless
a limited number, among whom De Boissiere and Montagu1 have de
scribed tertiary manifestations consisting of ulcers, bone pains, throat
ulcerations, lupoid ulcerations of the face and nose, gummata, enlarge
ment of the tibia, synovitis, dactylitis and “soki“ (small granuloma on
the sole, occasionally on the hand (De Boissiere)), bearing resemblance
to the late manifestations of syphilis, and encountered months or even
years after the primary invasion.
The subjective symptoms in yaws consist of a variable degree of
pruritus, and occasionally some spontaneous pain and tenderness; but,
as a rule, the yaw itself is not at all sensitive, and the tumor may be
touched with acid even with impunity (Manson).
Etiology and Pathology.—The disease is limited to tropical
countries, being endemic in certain regions; it is seen chiefly in the
black races, and in both sexes and at all ages, but is most common in
children.2 It is contagious and inoculable, and as in most diseases
of this class it is seen most frequently in those in poor health and living
unhygienically. One attack is, as a rule, protective. The point of in
oculation is almost always extragenital, and quite frequently on exposed
parts. It is conveyed by direct contact with the secretion from a yaws
lesion, by the contact of clothing, mats, or other agencies in a house
infected with the disease, from the dust in a village infected, and through
the bites of flies and other insects (McCarthy). The malady is un
questionably due to a micro-organism, but there has been as yet no uni
formly definite finding. Breda found a bacillus, Pierez, Nicholls, Watts,
Modder,3 and also Powell found cocci, and the last, as well as Haffkine,
found an yeast, but further confirmatory observations and experimental
investigations as to these have not been as yet forthcoming. Castellani
has found a spirochæte present in the lesions, which he believes to be
the cause of the disease; to this organism he has given the name of Spiro-
chæta pertenuis. While it closely resembles the spirochæta of syphilis,
it is considered by him, as well as by Blanchard, Mesnil, and others, as
morphologically different; Ashburn and Craig also confirm its etiologic
importance, and while considering it distinct, could not distinguish it
morphologically from the Spirochæta pallida. Other observers, among
1 Montagu, “Tertiary Yaws,” Jour. Trop. Med., June, 1910, p. 161.
2 McCarthy states that in a series of cases 113 were between one and five, 106
between five and ten, 54 between ten and fifteen, 21 between fifteen and twenty, 43
between twenty and thirty, 35 between thirty and forty, and 59 over forty years.
3 Modder (loc. cit.) grew and cultivated a micrococcus in acid media; growth ceased
in alkaline media.
FRAMBESIA
855
whom is Macleod, have either failed to discover any microbic factor, or
have considered those seen as the usual accidental contaminations to be
found in such formations.1
There seems no question, from an impartial study of the disease
and its literature, that it is one sui generis, and this view is held by the
various prominent writers cited in the text and in the literature refer
ences given. There still remain, however, a few observers, among whom
the most prominent are Hutchinson and Scheube, who believe it to be
syphilis modified by unknown conditions. Castellani does not consider
that the finding of spirochætæ has any such import. The experiments
by Neisser, Baermann, and Halberstädter in apes prove, moreover, that
syphilis does not protect from yaws, nor yaws from syphilis; and this is
fully in accord with the clinically observed facts.
The anatomy of the yaws lesion has been studied by Charlouis,
Pontoppidan, Rat, Breda, Jeanselme, Macleod, Pernet, and others.
The findings indicate, as suggested by the clinical picture, that yaws
belongs to the infective granulomata, and are very similar, in the main,
to those of lupus vulgaris, except that there are no giant-cells (Breda).
There is (Macleod) marked cellular infiltration of the corium, involving
all its parts except probably hair-follicles, sebaceous glands, and coil-
glands; and marked proliferation and downgrowth of the interpapillary
processes so great in the older lesions as to resemble condyloma acumina-
tum. Some observers believe (Rat, Pernet), that the peculiar frambe-
sial character of the lesion is probably merely the result of secondary
microbial infection from without.
Diagnosis.—The disease is to be distinguished chiefly from syph
ilis, with which it is most likely to be confounded—by the absence of in
duration of the inoculative lesion, of distinct or pronounced glandular en
largement (not always reliable), and of the usual associated lesions of the
mucous membrane of that disease. Daniels states that there is no resem
blance to primary or secondary syphilis and that it shows none of the asso
ciated lesions of that disease. It would certainly seem that the uniformly
prevailing peculiar frambesial or fungoidal character of the eruption,
developed out of pre-existing papules, nodular lesions or patches, with
an acid secretion, and covered with a crust is quite different from any
eruption of syphilis; in the latter disease a frambesiform character may
be an accidental condition in some lesions, but never a distinct charac
teristic of the eruption as a whole. To the trained eye, the histologic
differences would be of value in the differentiation.2 The Wassermann
1 Robertson (“Frambœsia Tropica”), Trans, of Eighth Session Australasian Med.
Cong., 1908, made examination of films prepared from the pus on the papules of 30
cases of yaws, and got the following results: Staphylococcus albus and aureus, and
streptococci in large numbers, and bacilli with square ends containing spores, and large
cocci in pairs, in all the films; and the Spirochæta pertenuis of Castellani in 12 of the
30 cases examined. Divisional forms of the Spirochæta pertenuis in 16 cases.
2 Macleod (Brit. Med. Jour., 1901, Sept. 21, and Practical Handbood of the Pathology
of the Skin, p. 200) gives the following summary of the histologic points which differ
entiate it from the other infective granulomata: It is distinguished from (1) actino-
mycosis and rhinoscleroma by the absence of their specific micro-organisms. (2) From
the lepromata by the absence of Hansen’s bacillus. (3) From mycosis fungoides by the
absence of “fragmentation” of the infiltrating cells, and of degenerative changes with
the formation of products of degeneration in the collagen and elastin; by the presence
856
NEW GROWTHS
test so frequently employed as a differential factor in suspected syphilis
is of no differential value here inasmuch as frambœsia cases usually
also give a positive reaction.
Prognosis and Treatment.—In mild and limited cases in sub
jects in good general health, the disease is at an end in six to eight weeks;
but in average cases the duration varies in children from three to six
months and in adults six to twelve months, and occasionally, with re
lapses, it may continue much longer. Europeans do not, according to
Graham, recover as quickly as natives. In those debilitated by ill-
health and dissipation, especially if cleanliness and other hygienic con
ditions are neglected, septic poisoning may ensue and death result.
The ulcers occurring in some cases may exceptionally be persistent
and rebellious to ordinary treatment.
There seems to be considerable unanimity as regards the curative
value of mercury and the iodids, along with other remedies which may be
indicated by the patient’s general health. Alkaline treatment has also
had a few advocates, Modder especially commending it. Strong,1
Cockin,2 Alston3 and Rost4 had rapidly successful results from salvarsan.
Of importance, as may be inferred, are improved hygienic conditions,
and good nutritious food. The external treatment consists in cleanliness
and the free use of antiseptic lotions, such as of boric acid and corrosive
sublimate, and mercurial ointments. Stimulation or mild cauterization
of the more obstinate lesions or patches is sometimes advisable. Per
sistent ulcers, when not responding to the usual remedies, may require
erasion with the curet.
Thorough disinfection of clothing, room, and house is of essential
importance in limiting the spread of the disease.
of the epidermal changes peculiar to yaws. (4) From tuberculosis, apart from the
tubercle bacillus, by the absence of the characteristic architecture with its giant-cells,
daughter plasma-cells, more marked disintegration of the fibrous stroma, and complete
disappearance of the blood-vessels. (5) From syphilis by the following details, which,
considered collectively, strongly suggest that yaws and syphilis are different histologic
entities: (a) Cellular infiltration: plasma-cells not so definitely arranged in rows or
clustered round the blood-vessels as in syphilis; no large multinuclear cells (chorio-
plaques), or true giant-cells, or intracellular hyaline degeneration noted in yaws, (b)
Fibrous stroma: rarefaction of the collagen more marked than in syphilis, but no organ
ization or colloid degeneration found, such as occurs in syphilitic gummata. (c)
Blood-vessels: no distinct proliferative changes in the vessel-walls or endothelium, as
frequently occur in syphilis, (d) Epidermis: marked proliferation and downgrowth
of the epithelium, with great thickening of the horny layer (due to hyperkeratosis or
parakeratosis) are characteristic features of yaws, while they are unusual in syphilis.
1 Strong, München Med. Wochenschr., 1911, lxviii, No. 8, p. 398, and Philippine
Jour. Sci., vol. v, No. 4.
2 Cockin, Jour. Trop. Med., Sept. 16, 1912, p. 277 (used it successfully in 22 cases
at the Yaws Hospital St. George’s, Grenada, W. I.).
3 Alston, Brit. Med. Jour., Feb. 18, and March 18, 1911, pp. 360 and 618; abs. in
Jour. Cutan. Dis., 1911, p. 515 (had good results from salvarsan and also favorable
influence with the serum from the salvarsan treated cases).
4 Rost, Munich, Med. Wochenschr., April, 1912, p. 924 (has had, in the West
Indies, almost uniform success with intramuscular injection of oily emulsion of salvar-
san—in most instances a cure resulting from one dose).
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |