| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
Macular Syphiloderm (Synonyms: Macular syphilid; Eryth-
ematous syphiloderm or syphilid; Syphiloderma maculosum; Syphilo-
derma erythematosum; Syphilis cutanea maculosa; Roseola syphilitica;
Exanthematous syphiloderm or syphilid).—This is usually the earliest
and most common of the secondary syphilitic cutaneous manifestations,
appearing commonly about six to eight weeks after inoculation, although
its appearance occasionally is somewhat later. It is generally distributed,
being most abundant, as a rule, on the sides of the trunk and axillary folds,
the umbilical region, the neck, and the flexor aspects of the arms. The
palms and soles also generally show numerous lesions, with often in some
a tendency to become maculopapular or papular. The face and dorsal
11 have never been able to convince myself that the nail changes in syphilis—
except those dependent upon or associated with eruptive lesions—present any special
diagnostic characteristics or condition which might not occur with or in the wake of
other constitutional diseases of a similarly grave and prolonged character. Others are,
however, not of this opinion. The reader interested in this subject is referred to the
general literature references under “Diseases of the Nails,” and also to a recent paper by
Adamson and McDonagh, Brit. Jour. Derm., 1911, p. 68, who in reporting two unusual
forms of syphilitic nails, give a good brief résumé (with good illustrations).
Plate XXII.
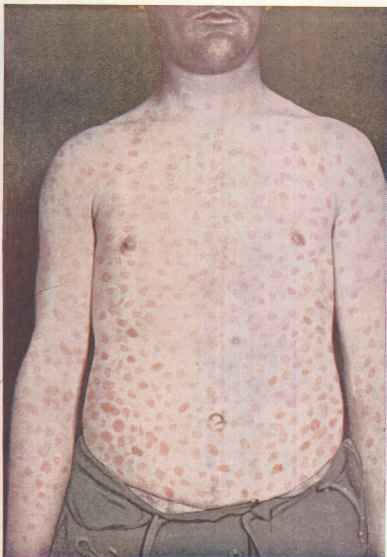
Macular syphiloderm, with some maculopapules on the lower part.
SYPHILIS
777
surface of the hands and feet frequently escape, although ill-defined
papules may sometimes be seen associated at the corners of the mouth
and at the nasolabial folds. The eruption may come out at once, or
gradually for a period of several days or longer, and, especially in in
stances of sudden outbreak,,is often preceded and for a time accompanied
with febrile action. In many of these latter cases a hot bath or violent
exertion or excitement often seems to be the immediate exciting factor.
The eruption consists of small or large, commonly pea- or bean-
sized, rounded or irregularly shaped, sometimes slightly raised, macules,
which, when well established, do not entirely disappear under pressure.
They show no disposition to crescentic or other peculiar shapes, although
in a few instances there are associated maculopapular or papular lesions
about the mouth, chin, and neck, and which may exhibit a tendency to
annular configuration (annular or circinate syphiloderm). At first the
color of the macules is a pale pink or dull, violaceous red, later, after sev
eral days or a week, becoming yellowish red or coppery. The efflorescences
are usually profuse, frequently crowded, but rarely forming coalescing
areas; often they are faint, and do not show clearly until the surface
has been exposed for several minutes—cold always makes the eruption
stand out more boldly. In cases in which the lesions are of a violaceous
tinge the skin is given a marbled look, especially when exposed to a cool
atmosphere. In some cases, instead of an abundance and closely
crowded, the macules are present in scanty number and widely scattered,
and could readily escape observation. In fact, in quite a number of
instances it is so mild that patients are first made aware of its presence
by the physician, who, led by the existence of suspicious sore throat,
mucous patches, or the initial sore or glandular swelling, for one or all of
which he may have been consulted, makes a general examination of the
surface. There are no subjective symptoms.
After persisting for one to several weeks, it gradually or somewhat
rapidly disappears, usually without desquamation, although slight
scaling or exfoliation is not uncommon in those macules which tend
to papular development, and which is not unusual with lesions on the
palms. Slight or moderate brownish-yellow pigmentation may, in some
cases, remain for some weeks or longer. Occasionally there may be a
slight recurrence, in which the macules are usually scanty in number
and somewhat larger than ordinarily, and sometimes tend to annular
configuration (annular or circinate syphilid).
In some instances many of the lesions of the macular eruption show
a tendency toward papular development, usually reaching a midway
stage, forming maculopapules; and occasionally this occurs with almost
the entire eruption, so that it is more clearly designated maculopapular
in type. Even if this tendency does not present, it is not uncommon
to find a few such lesions in the palms or soles and about the genitalia
or anus, in the latter two situations often becoming well-developed
papules, which may become macerated and moist. The macular syphilo-
derm disappears rapidly under specific constitutional remedies.
The diagnosis of the macular syphiloderm is rarely attended with
difficulty, inasmuch as it is commonly associated with other syphilitic
778
NEW GROWTHS
manifestations, such as a few or more scattered maculopapules or
papules, sore throat, mucous patches, moist papules about the anus,
falling of the hair; and, in most cases, the chancre is still present. The
presence or absence of such concomitant symptoms is of greatest value in
the diagnosis. It is to be distinguished chiefly from measles, rötheln,
tinea versicolor, and some drug eruptions. Measles is to be differentiated
by its catarrhal symptoms, fever, crescentic and blotchy character, and
the situation of the eruption, all of which differ materially from those
of the macular syphiloderm. Too much stress is not, however, to be
placed upon the febrile action, as this sometimes may be quite sharp in
syphilis. In rötheln there are small, roundish, confluent, pinkish or
reddish patches, with no tendency to pigmentation, and which are of
short duration; there is, moreover, usually evidence of its epidemic char
acter, and slight catarrhal symptoms, as in measles. The erythematous
drug rashes sometimes following the ingestion of copaiba, cubebs, bella
donna, opiates, etc, are a much more vivid red or scarlet, and are, as
a rule, quite itchy and of short duration. The evanescent wheal of urti
caria, with the accompanying itching, and the punctate scarlet redness of
scarlatina, are so unlike the macular syphiloderm that confusion with
these diseases is scarcely possible. The differentiation from tinea
versicolor is mentioned under the latter disease.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |