| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
ORIENTAL SORE1
Synonyms.—Delhi boil; Delhi sore; Oriental boil; Kandahar sore; Pendjeh sore;
Natal sore; Aleppo boil; Biskra button; Gassa button; Puru; etc. Fr., Bouton d’Alep;
Clou de Biskra; Ger. Orientbeule; Beule von Aleppo.
Definition.—A specific granuloma of the skin, endemic within
certain limited areas in warm countries; characterized primarily by a
1 Valuable literature: Murray, Trans. Epidemiological Soc, London, 1882-83, vol. ii,
p. 90 (with illustrations); Altounyan, Jour. Cutan. Dis., 1885, pp. 161 and 173; Riehl,
Archiv, 1886, p. 805; Hirsch, Handbook of Geographic and Historic Pathology, Syden-
ham Soc. ed., 1886, vol. iii, pp. 668-683, with bibliography almost complete to 1884;
Riehl and Paltauf, Archiv, 1886, vol. xiii, p. 805, etiology and anatomy, with review of
previous investigations; Leloir and Vidal, Traité descrip. des mal. de la peau, first and
second parts, 1890, 1891; Matas, Morrow’s System, vol. iii, (Dermatology), p. 708;
Auché and Le Dantec, Archiv Clin. de Bordeaux, Oct., 1894—abs. Brit. Jour. Derm.,
1895, p. 98 (bacteriologic, with review of other findings); Unna, Histopathology (with
846 NEW GROWTHS
papule, gradually enlarging by peripheral and subjacent infiltration,
with scaling or crusting, and which usually, sometimes with an inter
vening furunculoid stage, slowly breaks down and develops into an
indolent ulcer.
It is difficult to give an inclusive definition of this malady, if all
the various cases reported and described as such are true examples
of it. The differences can only be explained on the assumption of the
influence of environment, nutrition, hygienic conditions, and individual
resisting power. Errors in diagnosis are doubtless responsible for some
of the discrepancies.
Symptoms and Character.—There is a quiescent inoculation
period of from three days to one or more months. The lesion appears
as an itchy red papule. It gradually increases to the size of a pea or
small grape, usually flattened, becoming hard and more vascular. It
tends to become scaly, more especially in the central portion where it
later generally shows a crust formation with sometimes slight depression.
If the crust falls off or is scratched
off, a shallow erosion or ulcer is dis
closed. From the central necrotic
portion there may be some serous
oozing, changing to a seropurulent
character. It is chiefly of this
that the crust is composed. It
may continue in this manner, and
after a long while, commonly some
months, with usually an interven
ing ulcer formation, gradually heal
and disappear; or it may become
distinctly furunculoid, gradually
break down, discharge, and de
velop into an ulcer. While a
rather distinct, sharply cut, indo
lent ulcer is a common termination,
which finally heals and leaves a pronounced scar, the growth may con
tinue as a scaly or crusted nodule, and eventually disappear by desicca
tion, exfoliation, and absorption, with insignificant scar or atrophic
mark. It is not unusual for the “sore” to consist primarily of two, three,
or more closely aggregated papules, which, as they grow, become solidly
crowded or coalescent; the further development being as already de-
pathologic references); J. H. Wright, Jour. Med. Research, 1903, p. 472; and Jour.
Cutan. Dis., 1904, p. 1 (bacteriologic, with illustrations); Cox, Indian Med. Gaz., 1904,
p. 56 (clinical); Marzinowsky and Bogrow, Virchow’s Archiv f. Path. Anat., 1904, vol.
clxxviii, p. 112 (etiology); Mesnil, Nicolle, and Remlinger, Compt. rend. Soc. de Biol.,
1904, lviii, p. 167 (bacteriologic); James, Scientific Memoirs by Officers of the Medical
and Sanitary Department of the Government of India, Calcutta, 1905, New Series, No.
13 (chiefly bacteriologic); Malméjac, Echo méd. du Nord, 1905, p. 103 (treatment);
Strong, Philippine Jour. Sci., Manila, 1906, p. 91 (a good résumé of bacteriologic find
ings with references); Billet, Bull, de la Soc. de Path. Exot., Paris, 1909, vol. ii, No. 2
(patient, a soldier, with five sores, who had returned from Biskra); Darling and Connor,
Jour. Amer. Med. Assoc, 1911, April 20, p. 1257 (case in Canal Zone—3d case to date—
history of fly bite); and Darling, “Oriental Sore,” Jour. Cutan. Dis., 1911, p. 617 (gives
a good historic review); Howard Fox, Correspondence, ibid, 1912, p. 206 (with
pertinent excerpts from letter from W. B. Adams, of Beirut, and four excellent photo
cuts, two of which are here reproduced).
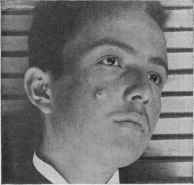
Fig. 202.—Oriental sore (courtesy of Dr.
W. B. Adams).
ORIENTAL SORE 847
scribed, although occasionally in this coalescent “sore” there is, as less
frequently, also, in the single lesion sore, a tendency to fungoidal granu
lations. On an average a fully developed Oriental sore is an inch or so
in diameter. While there is often but one, there may be several or more
distinct and sometimes quite widely separated formations. An Oriental
sore, when developed, is of a dull red color, is usually of sluggish nature
throughout its course, unless constantly knocked, irritated, or having
added an active pyogenic factor, when it may become much more in
flammatory, and quite tender and painful. The favorite regions are
the face, hands and forearms, and legs, but no part is exempt.
The ulcer, as remarked, is usually rather sharply cut, frequently
oblong and irregular in shape, with commonly some elevation and in
filtration of the surrounding border; the latter may or may not be un
dermined. It may discharge but slightly, so that it is continually
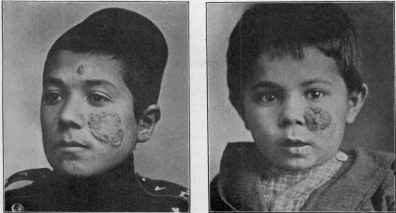
Fig. 203.—Oriental sore, a larger, Fig. 204.—Oriental sore, a larger
spreading, patch, with smaller lession and older lesion (courtesy of Dr. W. B.
on forehead (courtesy of Dr. W. B. Adams and Dr. Howard Fox).
Adams and Dr. Howard Fox).
covered with an adherent dry scab; or it is forever discharging abund
antly a pale yellow, watery pus, which adds to the discomfort of the
patient. After attaining a variable size the ulcer may remain stationary
for some time before the reparative process begins. In some cases,
however, the ulcer continues to extend, and may finally involve an area
of several inches or more, and persist; such instances doubtless furnishing
some of the examples of so-called “endemic ulcer,” “tropical ulcer,” etc
As a rule, however, after a variable period, of from two or three months to
a year or more, healing, sometimes more or less interrupted, sets in;
and this may be effected under the crust. In some cases the ulcer is still
extending peripherally whilst healing is progressing centrally. As
intimated, the character of the scar varies; it may be slight or almost
nil in some instances, whilst in others, more particularly when about
the face and joints, be extremely pronounced and disfiguring, and if
contraction occurs can give rise to considerable deformity. In fact,
848
NEW GROWTHS
the character, features, course, and cicatrix of the malady show wide
variations.1 There is no systemic involvement, but occasionally the
usual accidental complications of such ulcerative processes are noted,
such as lymphangitis, erysipelas, and the like.
Etiology and Pathology.—The disease is limited to certain
tropical countries, as the various names imply, but it is occasionally
met with elsewhere in travelers or immigrants from infected districts,
one such instance coming under my own notice. The malady is conta
gious, inoculable, and auto-inoculable; it is doubtless due to inoculation
through the media of infected laundry and other clothing and water,
breaks in the continuity of the skin being predisposing. Insects are
also probable carriers of the infection. It is thought that a poor condition
of the general health makes one more liable. In fact, some writers have
considered the malady of malarial origin. It is much more prevalent
in the autumn months. No age is exempt, but it is much more common
in childhood and adolescence and it is rare after forty-five. It is met
with in both sexes and in those of all nationalities. One attack seemingly
furnishes comparative immunity.
The lesion is admittedly the result of infection by some micro-organ
ism, and a number of investigators (among whom Laveran, Duclaux,
Heydenreich, Riehl and Paltauf, Leloir, Chantemesse, Wright, James,
Strong, and others) have been sanguine as to the import of their indi
vidual findings—variously, micrococci, streptococci, staphylococci, and
protozoa, or protozoa-like organisms resembling the Leishman-Donovan
bodies of tropical splenomegaly. These last (Wright, James, confirmed
by Mesnil, Nicolle, and Remlinger), also bear similarity to the organisms
found by Cunningham, Firth, Marzinowsky, and Bogrow.2 The evi
dence now seems pretty conclusive that the actual cause is a protozoön
—named Leishmania tropica3—gaining access through the intermediary
of insects.
1A few examples of this variation, especially as to its clinical characters: James (loc.
cit.) says “the appearances of some true Oriental or Delhi sores are by no means as char
acteristic as one would expect from the description given in books, and I found that civil
surgeons whose experience of the disease was considerable, were often unwilling to ex
press a definite opinion as to whether a given sore was really an Oriental sore or whether
it was an example of the ordinary chronic ulcers so common among natives of India.
When I say that the first examples of an Oriental sore seen by me in Delhi appeared, at
a superficial examination, to be more like a ringworm than anything else, and that I at
first considered another Oriental sore to be an ordinary ‘shoe-bite,’ it will be apparent
that I have felt a similar difficulty in diagnosis.” Sir Malcolm Morris (Derm. Soc’y,
Trans., Brit. Jour. Derm., 1902, p. 130, case demonstration of officer in India medical
service with Delhi boils on the arms), stated: “The lesions were in no sense of the word
boils, but rather resembled the verrucous forms of lupus of the extremities. Each
lesion was about as large as a shilling, and showed a raised, reddish, infiltrated swelling
of fairly firm consistence, over which the epidermis was thickened and warty. There
were no signs of ulceration or necrosis, which the patient, who was very familiar with
the disease, averred to be a later stage of the process.”
2 Strong (loc. cit.) believes the organisms found by him to be a form of blastomyces,
and that they seem similar to the bodies which have been found in ulceration of the
skin occurring in horses in the tropics suffering from blastomycetic infection, and that
these two diseases are probably identical or closely related species.
3 Nicolle and Manceaux, Annales de l' lnstitut Pasteur, Paris, September 25, 1910,
xxiv, have succeeded in cultivating the protozoön which they believe is responsible for
Oriental sore, and in reproducing the lesion in dogs and monkeys after a period of in
cubation ranging from 16 to 166 days. They find many points of resemblance between
ORIENTAL SORE
849
Microscopic examinations of the tissue of Oriental sore show that
it is a reaction of the skin against some virus of low virulence which has
produced granulation changes in the corium beneath and around the ulcer
(Macleod). The deposit of a tumor-like formation of granulomatous
tissue is the first and essential condition; the new tissue infiltrate destroys
and replaces all the structures of the true skin, and pressing upon the
epidermis causes it to atrophy and disappear, so that an ulcer results
(James). In a number of sections examined by Elliot, he found the
disease confined to the epidermis and corium extending through to the
subcutaneous tissue, with a distinct line of separation between the dis
eased portion and the surrounding tissue; the area of disease seemed
composed almost entirely of small, round, inflammatory or formative
cells and epithelial elements, and with no evidence of the disease begin
ning in the glandular structures. Riehl found giant-cells present quite
frequently. Unna looks upon it as a chronic serofibrinous inflam
mation of the whole cutis leading to central necrosis, softening, and
ulceration.
Diagnosis.—Its origin in and limitation to endemic districts, its
site, its beginning as an itchy papule, its growth into a desquamating
and crusted nodule, usually followed by ulceration, considered together
with its slow development and non-involvement of the general health,
are sufficiently characteristic for many of the cases. One could readily
imagine, however, how, especially in its early beginning, it might be
mistaken for several other affections, such as ecthyma, the primary lesion
or patch of frambesia, lupus, and other scrofulodermata, syphilis, and
the like.
Prognosis and Treatment.—Recovery always takes place,
usually after some months; but how much is due to the treatment
or to the natural course of the disease is difficult to say. Cleanliness
is all-important, and this, together with protection and possibly mild
soothing applications, is about all that many advise. By some, com
plete excision, cauterization, and the actual cautery (Murray) are vari
ously recommended for discrete lesions; the milder antiseptics are sub
sequently used. Painting the beginning lesions with iodin tincture
is commended (Hickman, Altounyan), and also mercurial applications
(Brocq, Vidal, Bard). Gaucher and Bernard obtained rapid results
from daily spraying (ten minutes) with boiled water, and the constant
application of compresses of the same; Malméjac strongly commends a
somewhat similar treatment: forcible spraying (150 to 200 c.c.) of the
sore with boiled distilled water at a high temperature twice daily for
Oriental sore and kala-azar; recovery from the latter protects the dog against infection
from the virus of Oriental sore and affords a partial protection to the monkey. The
evidence on hand suggests that the dog is the natural reservoir for the virus of Orien
tal sore. This animal thus seems to be the agent involved in the etiology of the
Leishmanioses. Wenyon, (“Parasitology,” vol. iv, 1911—abs. in Brit. Jour. Derm.,
1912, p. 166), concludes from his investigations (in Bagdad, etc) that the incubation
period is about two weeks and that the typical parasite—Leishmania tropica—can be
found except in the final healing stage; house flies collected from open sores nearly
always show the parasites in the gut; and mosquitos fed upon the sore are also found
to take up the parasite; doubtless flies and mosquitos act as carriers of the disease
and probably transmit it.
54
850
NEW GROWTHS
eight days, and then once daily, and compresses of dry aseptic gauze.
Large doses of quinin and arsenic are said (Besnier, Rankin) to have a
favorable influence in promoting the healing of the ulcers.1
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |