| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
vitiligo
Synonyms.—Leukoderma; Leukopathia; Acquired leukasmus; Acquired leuko-
pathia; Acquired achroma; Acquired piebald skin.
Definition.—A disease involving the pigment of the skin alone,
characterized by the development of several or more round, oval, cir
cumscribed, smooth, milky-white patches, tending to increase in size,
and exhibiting at their margin increased pigmentation.
Vitiligo and leukoderma are synonymous and interchangeable terms,
although some authors use the former for the acquired disease and the
latter for the congenital patchy loss of pigment, also designated partial
albinismus.
Symptoms.—In this affection there appear one or more small
round or oval white spots, most frequently primarily on the backs of
the hands, trunk, and face, these being favorite localities. In their earli
est beginning, which, as a rule, is insidious, they are usually unnoticed,
and often they escape observation until they are the size of a pea or
larger. It is not improbable that close inspection would show, in some
cases at least, that the first change was a hyperpigmentation followed by
atrophy of pigment and the development of the characteristic milky-
white spot. They tend to enlarge slowly, the neighboring skin showing
an excess of pigment, usually sufficient in degree to give it a much darker
color than obtains in the normal state. Indeed, in those of white skin
the darkened border is often considered by patients as the pathologic
condition, and the inclosed white areas looked upon merely as integument
not yet affected. In those of darker skin, however, and in negroes, the
change to the milky-whiteness is naturally the more conspicuous.
The spots are smooth on the surface and are not elevated above the level
of the skin, there being no changes other than pigment diminution with
surrounding increase in pigmentation. They vary in size from a scarcely
measurable spot to that of the palm and even larger. Their shape is
usually round or oval, sometimes irregular, owing to the spots becoming
1 Jefferiss, Lancet, 1872, vol. ii, p. 294.
VITILIGO
611
confluent; the edges are always convex, those of the pigmented bordering
skin concave. New spots may form from time to time and coalesce, and
may cover a surface of greater or less extent, forming large white areas
with irregularly rounded or scalloped borders. When such ensues, the
loss of pigment is much less noticeable than the surrounding hyperpig-
mentation. In color they are pinkish-white or dead milky-white. Both
to the touch and sight no difference from the normal skin is to be detected,
and none in reality exists, except that of the pigment changes. Within
the whitened areas the hairs may retain their normal color, but generally
they also share in the pig
mentary loss. The activity
of the sebaceous and sudori
ferous glands is not inter
fered with, and subjective
symptoms are not present.
The malady may be
extremely slight, only a
few spots presenting, or
they may be numerous, and
exceptionally may gradu
ally invade the entire sur
face, as in instances ob
served by Lévi, Hall, Hard-
away, Simon, and myself.1
While the affection shows
a predilection for the dor-
sum of the hand, the face,
neck, and trunk, and also
the genital and perineal re
gion, it may begin or occur
upon any hairy or non-hairy
part2 of the body. Occa
sionally there will be a few
spots on the face and hands
and one or several in the scalp, the latter making themselves known
by the whitening of hair growing thereon. Not an infrequent site
is around the eyes, surrounding them by a white band, which in the
negro produces striking disfigurement. The disease is characterized
by its slow course and by its chronicity, months and sometimes years
elapsing before it reaches conspicuous development. It may, after a
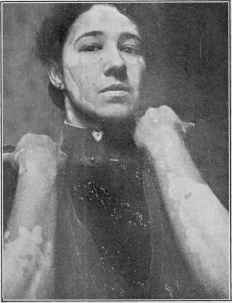
Fig. 144.—Vitiligo; patient a dark brunette
aged thirty; considerable increase in pigmenta
tion beyond the white vitiligo areas.
1 Lévi, “Recherches sur le Vitiligo,” Receuil de Mem. de Méd. de Chir. et de Pharm.
mil., 1865, p. 193 (3 cases); Hall, Louisville Med. News, 1880, vol. x., p. 148, records
the case of a dark mulatto who, with the exception of a part of the chin and a few small
patches on the hands, became completely white; Hardaway, Manual of Skin Diseases,
second edit., p. 280 (2 cases, 1 a white man and 1 a negro, with illustration of the negro,
p. 278); Simon (loc. cit.) noted a few instances of practically general involvement;
Stelwagon, Amer. Jour. Med. Sci., July, 1885 (white man); and Trans. College of
Physicians, Philada., 1894 (negro).
2 In 31 instances noted by Lévi it began on the scalp in 6 cases, epigastric region in
4, forearm in 3, scrotum in 3, breast in 3, ends of the fingers in 2, hands in 2, face in 2,
back in 1, arm in 1, penis in 1, and at the site of scars in 2 (region not stated).
6l2 ATROPHIES
time, remain stationary, and in rare instances retrogresses, but, as a rule,
however, it is progressive, although its increase is often so slow that it is
scarcely perceptible. With some exceptions it can be stated that when
the normal pigment has once been lost, it does not return. When a larger
area has been deprived of its pigment by the coalescence of several or
more patches, and the coalescing hyperpigmented borders may not have
completely disappeared, the brownish islets remaining are taken for the
diseased condition and may lead to errors in diagnosis. Season of the
year has no material influence, if any, upon the morbid process, but
during the summer months the discoloration is more noticeable and

Fig. 145.—Vitiligo; showing also the surrounding hyperpigmentation. A common site
for the patches.
disfiguring, owing to the increase in depth of coloring of the bordering
pigmentation, which is due to the greater action of the actinic rays and
to the direct exposure to the sun, the whitened areas being but slightly,
and usually not at all, influenced. As a result the white looks relatively
more pronounced, the surrounding pigmentation is increased, and the
blemish, in consequence, more noticeable. In women of naturally very
light skin the patches give rise to but little annoyance except during the
sunny season, when, for the reasons stated, they become quite conspicu
ous. Not infrequently, however, considerable disfigurement results
when such regions as the face, neck, and hands are involved, even in the
VITILIGO
613
winter time, and proves a source of much mental worriment. The mal
ady in the negro is, of course, a striking one, and extensive milky-white
surface often results, examples of the disease in this race giving rise to
the occasional newspaper notices of a “negro turning white”; in a few
instances already referred to the change was in reality complete. At
no time during its course is the general health impaired, the malady
having no damaging influence, but, on the other hand, ill health from any
cause is apt to lead to further increase in the patches.
Etiology and Pathology.—The cause of vitiligo is unknown.
Although not common, it is not infrequent. A relationship to disease
of the suprarenal capsules has been suggested (McCall Anderson). It
occurs in males as well as females, and with, usually, about like fre
quency, although of Lévi‘s 37 cases 28 were men. It rarely begins before
the tenth, nor after the thirtieth, year. According to statistics, it is
more frequent in tropical countries (India) and in the dark races. Forel1
states that it is very common in certain districts of Columbia, where
the natives are mostly of mixed negro, Spanish, and Indian blood. , It is
not frequent, but still not at all rare, in our own country. Some observ
ers are of the opinion that extremes of heat and cold both seem of pos
sible etiologic import. At times it is hereditary. It is undoubtedly to be
looked upon as a neurosis, and of more frequent occurrence in neurotic
individuals. Often however, absolutely no history of systemic disturbance
can be obtained. In some instances severe illness, such as ague, scarlatina,
and typhoid fever, would appear to exert an influence. There scarcely
seems a doubt that the nervous system plays an important part, as shown
by the observations of Fèvre, Wyss, Fournier, Schwimmer, Bulkley, and
others.2 Extensive cases resulting after fractures and injuries to nerves
have been reported. It is not infrequently associated with alopecia
areata, and occasionally with morphea. Its occurrence in Graves’
disease has also been noted (Trousseau, Raynaud, Rolland, Bramwell,
Dore, and others).3 The malady has been occasionally observed to
begin at the site of an injury, from pressure, ulcerations, condylomata
lata, and burns. Shepherd has noted the disease in one instance to
start from the pressure of a collar-stud and another from the spots
left after burning warts. Hebra believed that not infrequently the
first area arose in close proximity to a previously existing pigmented
mole. The so-called pigmentary syphilid (q.v.) is thought by some
observers to be a vitiligo (vitiligo syphilitica) starting at the sites of
former macules.4
The very earliest pathologic change to be noted in vitiligo is, I
1 Forel, Munch, med. Wochenschr., 1897, p. 1009.
2 Quoted by Leloir, Twentieth Century Practice, vol. v, p. 848; Lebrun, These de
Lille, 1886, was also of the opinion that other nervous disturbances were usually to be
found.
3 Dore, “Cutaneous Affections Occurring in the Course of Graves’ Disease,” Brit.
Jour. Derm., 1900, p. 353.
4 That syphilis has, however, any etiologic relationship to true vitiligo, as Marie
and some others suggested, seems, in my judgment, without the slightest tangible
foundation. Thibiérge (Annales, Feb., 1905, p. 128), and others give ample negative
evidence, as for example the existence of vitiligo in those whose syphilis is contracted
subsequently.
614
ATROPHIES
believe, an increase of pigment,—a hypertrophy instead of an atrophy,
—followed by diminution or atrophy, and in the further spread of the
lesions the same pathologic steps are gone through. Anatomically, as
to be inferred, the whitish spots are seen to be wholly devoid of coloring-
matter, whereas the surrounding brown discoloration shows hyperpig-
mentation. The atrophy of the terminal nerves noted by Leloir1 and
Chabrier has not, up to the present, been confirmed.
Diagnosis.—The diagnosis is usually not difficult. In extensive
cases, where the pigmented portions are the more striking, it might be
confused with chloasma, but it may be differentiated from the latter by
the fact that the white areas have convex borders, and the pigmented
part would naturally show the reverse,—concave,—while in chloasma
these would be reversed, the chloasma pigmentation being irregularly
round or diffused. Moreover, chloasma, as generally encountered, is
upon the forehead and sometimes on other parts of the face as well,
but it is rare elsewhere. Under the same circumstances it could possibly
be confounded with tinea versicolor, but the same points as regards the
borders would obtain here also, and when it is borne in mind that in
tinea versicolor the patches are usually furfuraceous, of a yellow or fawn
color, and the intervening skin is normal in appearance, no error should
arise; furthermore, the microscope will reveal the presence of the micro-
sporon furfur, the causative agent in the latter malady. Another dis
ease which, upon casual inspection, it resembles to some extent is mor-
phea. The latter, however, is associated with structural changes in the
skin, while in vitiligo there exists only an absence of pigment in circum
scribed patches, and which are on a level with the skin, whereas in mor-
phea the patches may be somewhat elevated above it, or sometimes
slightly depressed, and the seat, as disclosed to the touch, of other
distinct changes. Occurring in tropical climates, it is at times con
founded with the white patches of true leprosy. Indeed, according to
Minch, vitiligo is somewhat widely distributed in Turkestan, and is
considered contagious by the Sarts; affected persons are segregated and
kept with the lepers within special inclosures (Ziegler)—a most extra
ordinary procedure unless, as is possible, they are held as simple sus
pects temporarily. In this type of leprosy, however, the whitish patches
are anesthetic and there are structural changes in the skin and constitu
tional symptoms present, which is not the case in vitiligo. Partial
albinism, which, as already remarked, is often termed leukoderma, is,
reality, similar to this malady except that the normal pigment is absent
from birth; it is, therefore, a congenital condition, whereas vitiligo de
velops during life.
Prognosis and Treatment.—The outlook for recovery from
the malady is not very encouraging. The spots tend, as a rule, to in
crease quite slowly in size for a number of years, and the skin over parts
of the body may become entirely deprived of pigment. In such instances
1 Leloir, “Contribution a l‘Etude des affections cutanées d‘origine trophique,”
Arch, de Physiol., 1881, p. 397; see also interesting clinical and histologic paper by
Marc,“Beiträge zur Pathogenese der Vitiligo und zur Histogenese der Hautpigmen-
tirung” (with review and references), Virchow‘s Archiv, vol. cxxxvi, p. 21.
VITILIGO
615
the last remnants are a few islets of pigmentation, the remains of por
tions of the pigmented borders, which also gradually fade away. Gen
eral involvement is, however, extremely rare. Not infrequently, after
progressing for some years, it comes to a standstill, and exceptionally it
retrogresses and disappears. Fortunately, the disease gives rise to no
symptoms other than the disfigurement.
It is questionable how far treatment influences its course. The con
tinued administration of arsenic, along with tonic remedies, if indicated,
has in some instances, it is believed, influenced it favorably. Duhring
considers this the most valuable remedy, and in some cases under my
care the progress of the malady seemed to be stayed. Pilocarpin has
likewise been suggested, and also thyroid; recently good effects from
suprarenal gland have been claimed. In young patients cure has been
stated to follow the use of potassium bromid internally, along with alka
line baths (Besnier and Doyon). General galvanization and the use of
the battery with the positive electrode to the back of the neck and the
other over the patches has been credited with favorable influence. The
general condition of the patient should receive attention, and measures
directed toward bringing the health up to the normal state adopted. In
recent years I have prescribed most frequently both arsenic and supra
renal gland in this disease, and exceptionally with seeming benefit.
Externally the white patches can be rendered less conspicuous, and
the disfigurement lessened, by reducing the pigmentation of the border
by the means used in the treatment of chloasma. Recently Savill1
successfully employed for this purpose pure phenol, painting it over;
the outer epidermis subsequently exfoliating, with a disappearance of
the discoloration. In cases of sensitive skin it would be advisable to
apply it at first weakened with alcohol, and to limit the application to a
small area. In addition to endeavoring to lessen the bordering pig
mentation, stimulating applications to the white patches, with a view to
producing hyperemia and consequent pigment deposit, can, if thought
advisable, be practised. One of the best for this purpose is the negative
electrode of a galvanic battery, with a current of 2 to 5 milliampères.
It should not be held on the same spot for more than one to several
minutes, so as to produce redness, but to avoid too great effect, otherwise
some damage might be done. The application of the tinsel or metallic
brush, either with the faradic or galvanic battery, and the high frequency
electrode will likewise produce redness. The actinic rays, as well as
heat rays, of the various lamps will also tend to produce pigmentation.
Mustard, in the form of a plaster, cantharides, burning glass, and similar
measures are also resorted to. The white patches may be masked by
coloring, from time to time, with walnut juice or similar stain, or with
an extremely weak tincture of iodin or like substance.
1 Savill, Brit. Jour. Derm., 1898, p. 99.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |