| MEDICAL INTRO |
| BOOKS ON OLD MEDICAL TREATMENTS AND REMEDIES |
THE PRACTICAL |
ALCOHOL AND THE HUMAN BODY In fact alcohol was known to be a poison, and considered quite dangerous. Something modern medicine now agrees with. This was known circa 1907. A very impressive scientific book on the subject. |
DISEASES OF THE SKIN is a massive book on skin diseases from 1914. Don't be feint hearted though, it's loaded with photos that I found disturbing. |
SUPPLEMENTARY SECTION
FOR PRESENTATION OF A FEW DISEASES OF THE ADJOINING MUCOUS MEMBRANES NOT ELSEWHERE CONSIDERED
The mucous membranes in proximity to and adjoining the skin are quite frequently the subject of diseases corresponding to, and existing conjointly with, those of the latter. These have, to a great extent, been already referred to in connection with the individual cutaneous maladies, such as eczema, lichen planus, pemphigus, erythema multiforme, lupus vulgaris, syphilis, and others. It is the purpose to describe here briefly several other affections of the tongue, vermilion of the lips, and contiguous mucous membrane which come from time to time under dermatologic inspection.1 For other diseases of the tongue and oral cavity the reader is referred to special works on the subject.2
LEUKOPLAKIA
Synonyms.—Leukoplakia buccalis; Leukokeratosis buccalis; Leukoma; Leuko-plasia; Ichthyosis linguae; Tylosis linguae; Psoriasis of the tongue; Smokers’ patches; Chronic superficial glossitis; Fr., Leucoplasie; Plaques opalines; Plaques blanches des fumeurs; Plaques blanches de la bouche.
Definition.—A disease of the mucous membrane of the buccal cavity, commonly of the tongue, characterized by one, several, or more rounded, irregularly shaped or diffused, whitish patches, often more or less thickened, with sometimes a tendency to fissure. Although this not infrequent malady was occasionally alluded to in older writings, Bazin (1866) and his pupil Debove were the first to give a clear description, followed by the classic presentation by Schwimmer,3 Vidal,4 Leloir,5 Besnier and Doyon.6 These and other contributions have firmly established the individuality of the affection, and demonstrated that it is not a manifestation of psoriasis or a symptom or conse quence of syphilis, but that it may often arise and exist independently of these and other maladies.
Symptoms.—The earliest evidence of a leukoplakia patch is a slightly increased redness, sometimes with a bluish tinge, which is often so trifling as to be recognizable only on close inspection. Sometimes it has a somewhat thinned or abraded look. Oc casionally there is also a scarcely perceptible accentuation of the papillae, peripherally as Well as less commonly on the surface of the spot itself. At this time there is often some sensitiveness to hot and acid foods. This stage of the malady, which lasts a variable time of weeks or months, frequently escapes observation, the first sign recog-
1 Fordyce, “Some Affections of the Oral and Nasal Cavities which Are Related to Skin Diseases,” New York Med. Jour., March 6, 1909, p. 465, gives a serial review of these and other various conditions showing mucous membrane involvement.
2 See the admirable and largely illustrated monographs by Butlin and Spencer, Dis eases of the Tongue, Cassell and Company; Mikulicz and Kümmel, Die Krankheiten des Mundes, Jena; and Zinsser, Diseases of the Mouth (translated and edited by J. B. Stein, Rebman Co., New York).
3 Schwimmer, Archiv, 1877, p. 511 (with review of the subject, references, and 4 colored case illustrations).
4 Vidal, Union méd., 1883, vol. xxxv, pp. 1 and 37.
5 Leloir, Arch, de Physiolog., 1887, vol. x, p. 86 (with 6 colored histologic illustra tions).
6 Besnier and Doyon’s French translation of Kaposi’s treatise.
1203
1204
SUPPLEMENTARY SECTION
nized being the white or opaline spot into which it slowly evolves. This consists of a rounded, ovalish, or irregularly shaped patch of a faint pearly, bluish-white, or pale milk color, usually on a level with the surrounding surface, from which it is sometimes bounded by a narrow line of hyperemia. Instead of a well-defined area, it quite often first presents as one, several, or more short or long, straight or crooked, pale white lines, which may be close together and more or less parallel, of the same or different lengths; or instead of lines there may be scattered or grouped pin-head to small pea-sized white spots. Contiguous lines, points, or spots may gradually coalesce and form larger areas. There may also be slight papillary hypertrophy. This stage of the malady may continue for some time or almost indefinitely, generally with a tendency to trifling thickening of the affected membrane. There may be a tendency to trifling exfoliation. It is not uncommon, moreover, to find the affected surface, as well as other parts of the tongue, traversed to a variable degree with superficial or deep trans-
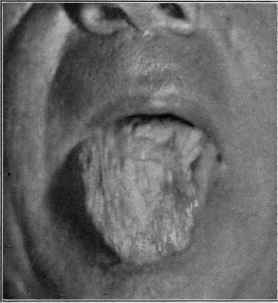
Fig. 324.—Leukoplakia, of slight development, chiefly short streaks and small spots, in a man aged fifty, of several years’ duration; also a pale, somewhat diffused, milky color of the main portion of the tongue, and some furrowing; contracted syphilis when aged thirty-five, but has had no manifestations for years.
verse and longitudinal grooves. These are the so-called “smoker’s patches,” although this term is likewise applied to the more advanced types also. The extent involved may be small, but one or several patches being seen, or a greater part of the tongue, or of the inside of the cheeks or other parts of the oral cavity, may be involved. In ad vancing cases the symptoms become, in the course of months or several years, slowly more pronounced, the submucosa variably, often considerably, thickened, the surface rough, rugous, and desquamating, with often a tendency to superficial cracks through the dry, hardened white epithelial coating. The affected area is stiff and less elastic than the unaffected parts. New spots usually present after variable periods, going through the various phases already outlined. In many instances after a certain stage or extent is reached the malady continues at a stand, or progresses so slowly that prac tically but little change is noted from month to month or even year to year. The corni-fied, somewhat firmly adherent epithelium is rough, exfoliates, usually in small frag-
LEUKOPLAKIA
1205
ments, from time to time; it can be partly removed only with great difficulty. In other cases the plaques spread, become much thicker, rougher, and even nodular, with short
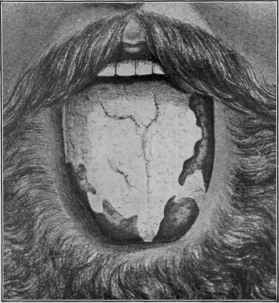
Fig. 325.—Leukoplakia of extensive development, in a man aged forty-five, and of eight years’ duration; has been subject of psoriasis for twelve years; never had syphilis (Schwimmer).
or long cracks, extending more or less deeply, and in places amounting almost to super ficial ulceration, giving rise sometimes to considerable pain and discomfort. Slight bleeding may occur now and then. The disease may occupy considerable surface. In
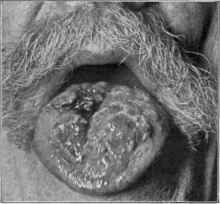
Fig. 326.—Leukoplakia, with development of epitheliomatous changes; patient aged
sixty-five.
still less favorable instances the deep fissures change to ulcerations, show considerable infiltration, and gradually, sometimes rapidly, develop into epithelioma, which in the
1206 SUPPLEMENTARY SECTION
graver cases sooner or later passes rapidly into a malignant type, with fatal termina tion. As in the earlier stages, there is in most instances in the well-developed malady sensitiveness to hot and irritating substances. The region most commonly the seat of leukoplakia is the tongue, especially the dorsal surface, anteriorly and laterally, but it may occur on any or all sections of this organ, and involve a portion or the greater part of it. The inside of the cheek is another favorite, but less frequent, situation, and the inner aspect of the lips, and even the vermilion border, especially at the commissures, may likewise be occasionally its site. Other mucous surfaces, as of the vulva, and even the glans penis (Krauss, Planz),1 are exceptionally the seat of similar formation. I have met with one instance in which it was limited to the urethral orifice, verging \ inch on to the glans, and one involving chiefly the prepuce, with hardening and contraction (kraurosis).
Etiology and Pathology.—The causes of leukoplakia are not clearly established. It is very rare in women, and is with some exceptions a development of middle life. Syphilis has always been considered of etiologic import, but it occurs frequently enough
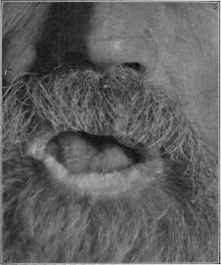
Fig. 327.—Leukoplakia—well marked on lower lip, slight on tongue.
in non-syphilitics to call this in question. Most of one’s patients with leukoplakia, it is true, have had syphilis, but such subjects naturally suspect any manifestations, and immediately seek advice, while those free from guilt in this direction are much less solicitous. Both Debove and Schwimmer met with instances of the disease in those who subsequently acquired syphilis. It is not improbable the mercurial treatment of syphilis may, by its invoking a mild, and though often scarcely perceptible, stomatitis, be a factor of some influence. There is no doubt about the aggravating influence of smoking, and so evident is this that this practice has been considered etiologic While its damaging, and probably, under some circumstances, its causative, action cannot be denied, yet the fact remains that the malady is also seen in those not addicted
1 Krauss, Archiv, 1907, vol. lxxxv, p. 137; Planz, “Ueber idiopathische Schleim-hauteleukoplakien mit besonderer Berücksichtigung der Leukoplakia Penis,” Dermato-log. Zeitschr., 1909, pp. 619, 710 (2 cases; review, and full bibliography); Bohac, “Ueber Leukoplakia und Kraurosis der Schleimkaut und der Haut,” Archiv, Jan., 1911, cv, p. 179 (3 cases involving glands and prepuce; 1 case in woman, involving mucous mem brane of the lip, with extension to the skin; general survey and review).
LEUKOPLAKIA
1207
to this habit. It has often been looked upon as a psoriasis and is sometimes seen as sociated with this malady, but it is also seen in association with similar scaly and other skin eruptions, attended with increased cornification; Schütz1 observed leukoplakia in 2 cases of tylosis and in 5 of scaly eczema. Whatever may be the essential initiative cause, there is no difference of opinion as to the aggravating and contributory influence of smoking, strong alcoholic drinks, hot, highly seasoned, irritating, and acid foods. Sharp, rough, and decaying teeth are also to be considered contributory. A factor of considerable import in my experience is gastric or gastrointestinal catarrh.2
The anatomic changes have been studied by most of the various observers already named, and by Fordyce, Pollitzer, Heidingsfeld, and others. There is, as is to be ex pected, but little divergence in the findings, although it is held by some that the earliest changes are in the superficial epithelium, and by others that these are secondary to an inflammatory process in the papillary region. There is found keratosis, with marked
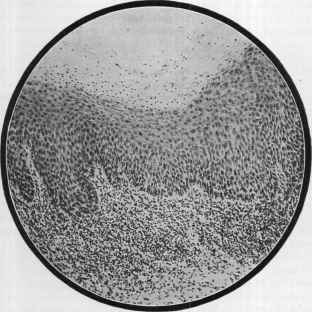
Fig. 328.—Leukoplakia, showing keratosis of the superficial layers of epithelium, and marked inflammatory changes in the subepithelial tissues (courtesy of Dr. J. A. Fordyce).
thickening of the superficial layers, thickening of the deeper strata, and down-growth of the epithelial processes, and in places there may be more or less obliteration of the papillae, with the subepithelial tissue showing inflammatory changes and infiltration of round cells. Finally, sclerotic changes may ensue in the submucous and deeper layers. Leloir found that the epitheliomatous changes started from the ulcerations and not from the unbroken hyperkeratotic parts. Fordyce’s3 examinations in instances of epitheliomatous development showed the new growth to belong to the tubular epi-
1 Schütz, “Ueber Leukoplakia oris bei Psoriasis und anderen Dermatosen,” Archiv, 1898, vol. xlvi, p. 433 (a good review with pertinent bibliography); Filarétopoulo, Jour, mal. Cutan., 1905, p. 81, also refers to the varied causes or associations.
2Hertzka, Deutsche med. Wochenschr., 1880, vol. vi, p. 154, met with the disease in several women in whom gastrointestinal catarrh seemed etiologic.
3 Fordyce, Morrow’s System, vol. iii, (Dermatology), p. 626.
1208
SUPPLEMENTARY SECTION
theliomata, with but little, if any, disposition to the formation of horny tissue. Heid-ingsfeld,1 in a case of long duration, showing as yet apparently no degenerative changes, found the leukoplakic condition to be distinctly pre-epitheliomatous in character— marked proliferation and down-growth of the epidermis and areas of degeneration, with a nest-like arrangement of the epithelium; a good wall of connective tissue separated it from underlying structures.
Diagnosis.—The beginning features, the history, and slow persistent course are characteristic. Leukoplakia of the tongue is readily recognized. It might possibly be confused with the mucous patch of early syphilis, but there is in the latter no tend ency to epithelial hardening, but, on the contrary, it is usually soft, with the surface film generally easily removed and a disposition to superficial abrasion, and not infre quently to more or less ulcerative action. The mucous patch is, moreover, of rapid formation, witE commonly, therefore, even though well developed, a history of short duration. Other symptoms of syphilis will, as a rule, be found. Lichen planus patches on the inside of the cheeks, a somewhat rare occurrence, may bear a suggestive resemblance, but they tend to present in irregular streaks or peculiar shape, especially on other parts of the mouth; in addition, lichen planus is rarely, if ever, for any length of time at least, limited to this region, but when occurring there, it is almost invariably with the eruption on some part of the cutaneous surface.
Prognosis and Treatment.—When well developed, the malady is persistent and rebellious. In the early stage of some cases abstention from smoking and irritating foods and drinks will halt its advance and sometimes promote its disappearance. The possibility of malignant development is to be kept in mind. In the treatment of the disease in its earliest existence the prevention of irritation from food, drink, or sharp or decayed teeth, together with the maintenance of good digestion and free action of the bowels, will often accomplish much, or at all events not infrequently stay its progress. The occasional use of mildly astringent and antiseptic mouthwashes is found of service. At this period application every day or two with glycerite of tannic acid, and every two or three weeks with silver nitrate stick, will sometimes prove beneficial. When epi thelial thickening has taken place, the same general plan can be advised, but, as a rule, no decided betterment is possible except from active cauterizing applications. These, if employed, however, should be used boldly and thoroughly, otherwise there is likely to result more harm than good. There seems to be considerable unanimity as to the value of thermocauterization, preferably with the galvanocautery. The latter has been in my hands of decided value in several instances. Vidal's favorite application was a 20 per cent, solution of chemically pure chromic acid, and this is also employed by others. Sherwell2 strongly commends the thorough and prolonged application of liquor hydrargyri nitratis, the surrounding parts being protected by absorbent cotton. Unna, Leistikow, and Schiff3 speak well of the application of a resorcin peeling paste, such as is used in acne, a thin coating being smeared over daily until exfoliation occurs, and the treatment repeated at intervals of a week or so.
Bockhardt4 states that if patients will abstain from smoking he can bring about a cure with an application, daily or every other day, of balsam of Peru, and frequently repeated (6 to 12 times daily) washing out of the mouth with a ½ to 3 per cent, salt solution; cure takes three months to two years, according to the case.
As to constitutional treatment, there is a difference of opinion as to the value of antisyphilitic remedies in those cases with a previous syphilitic history, and most observers are inclined to consider it of but little, if any, value, and that it may be even detrimental. With a few exceptions they have proved valueless in my experience. In such instances, however, when the disease has developed but a few years after the con-
1 Heidingsfeld, “Trans. Cincinnati Acad. Med.,” Amer. Medicine, March 23, 1901, p. 834. 2 Sherwell, Jour. Cutan. Dis., 1899, p. 185.
3 Schiff, Wien. klin. Rundshau, 1895, p. 113.
4 Bockhardt, Monatshefte, 1902, vol. xxxiv, p. 164.
TRANSITORY BENIGN PLAQUES OF THE TONGUE 1209
traction of syphilis, and is of rapid development, and especially in those in which there is a suspicion that some of the infiltration may be of a gummatous nature, these remedies, especially potassium or sodium iodid, should be tried. In the aggregate of cases I believe much more is to be accomplished by remedies directed toward any digestive or catarrhal gastrointestinal disturbance that may, and frequently does, exist.
FURROWED TONGUE
Synonyms.—Grooved tongue; Wrinkled tongue; Sulcated tongue; Cleft tongue; Fluted tongue; Ribbed tongue; Scrotal tongue; Lingua plicata; Fr., Langue plissée; Langue montagneuse; Langue scrotale; Ger., Gelappte Zunge.
Furrowed tongue is, in most instances, a condition to which some families seem especially prone. It is seen on the dorsal surface, and may consist simply of the deep ening of the central furrow, common to many persons, with one or several less distinct parallel linear depressions, or they may be so numerous and deep as to present a verita ble network of lines, depressions, and correspond ing elevations. When there is a natural or ac quired enlargement (macroglossia) of this organ, and the furrows are irregularly longitudinal, transverse, curved, and forked, the general aspect may be suggestive of a miniature of crowded valleys and mountains or sometimes of the convolutions of the brain. The surface of the depressions or clefts is usually smooth and free from fur. When deep, there is a tendency from time to time for minute particles of food to collect in them, undergo change, and produce irritation.
The condition, especially in its milder phases, is not very rare. It is in some cases congenital, with a family tendency, but is rarely of marked development in infancy or early childhood. In others it appears later in life, spontaneously or as the result of irritating influences and of various forms of glossitis and other diseases, some of which may be due to syphilis, hereditary or ac quired. Their formation is sometimes partly owing to, and made more pronounced by, oversize of the tongue, the organ kept somewhat crowded in its natural bed.
Excepting the appearances and the occasional irritation due to the collection of food-particles in the crevices, and the possibility of the irritation thus repeatedly pro duced being the starting-point of epithelioma, the affection has no significance. Treat ment is rarely sought, but in order to guard against the possible consequences men tioned, it is important that the mouth and tongue should be kept clean, using water freely, and from time to time mild antiseptic solutions, such as one of boric acid and myrrh, the furrows and crevices being separated so as to permit of thorough cleansing.

Fig. 329.—Furrowed tongue, with a moderate degree of macro-glossia.
TRANSITORY BENIGN PLAQUES OF THE TONGUE
Synonyms.—Exfoliatio areata linguæ; Pityriasis linguæ; Annulus migrans; Glossitis areata exfoliativa; Erythema migrans; Wandering rash; Ringworm-like patches of the tongue; Circinate eruption of the tongue; Fr., Desquamation aberrant en aires de la langue; Desquamation épithéliale de la langue (Gautier); Glossite exfoli-atrice marginée (Fournier, Lemonnier); Lichénoide lingual (Gubler, Vanlair); Eczéma en aires de la langue (Besnier); Eczéma marginée desquamitif de la langue; Ger., Flüchtige, gutartige Plaques der Zungenschleimhaut (Caspary); Landkartenzunge.
Brief mention or account of this rare and strange affection is to be found some years back, but it was not until the more recent clear and fuller descriptions by Bridou,
1210 SUPPLEMENTARY SECTION
Gubler, Caspary, Vanlair, Barker, Gautier, Unna, Colcott Fox, and others that the matter excited much attention. In our own country there is scant literature, cases having been reported by Kinnier, Hartzell, and Allen.1
Symptoms.—The malady shows itself as one or several small, pin-head-sized, grayish, well-defined, slightly elevated spots, of vesicular aspect, on the dorsum of the tongue and most commonly laterally and toward the tip. Exceptionally, as in one of Caspary’s cases here pictured, the under surface is also the seat of lesions. The patches spread peripherally, the central part tending to superficial exfoliation or desquamation, and becoming moderately or markedly reddened, often glossy, and sometimes present ing the appearance of a slight abrasion, and with apparently trifling depression. The patch is frequently of a brighter red toward the border. The peripheral spreading portion exhibits the grayish, pseudovesicidar aspect of the beginning central point. Sometimes there is a yellowish hue to the border, and sometimes bluish, but generally it is grayish, and even silvery white. Exceptionally, the spot is without the yellowish or whitish border. A patch ordinarily reaches the diameter of ½ inch, frequently greater, and then begins to disappear, the central portion first resuming the natural appearance. From one or two to ten days or more is commonly required for a patch to present, run its course, and disappear, and marked development and changes can occur in several hours. In many instances but one or two such areas are present at one time, new ones appearing from week to week or month to month as the old spots fade, and thus the malady may continue indefinitely. There are, however, generally periods of variable duration when the tongue remains entirely free from manifestations. When several are to be seen, from enlargement, coalescence may result, and a peculiar appearance be presented, giving rise to the term "geographic tongue” (lingua geograph-ica).
The plaques are usually well rounded, occasionally being somewhat irregular, the irregularity being doubtless due, as suggested by Unna, to the fusing of closely contigu ous beginning points at various parts of the border. Guinon saw 1 instance in which a plaque was more or less diffused along the median line. Spots near the side of the tongue sometimes finally become segmental or half-moon shaped, extension ceasing at the edge of the organ, although they may go beyond on to the under surface. As a rule, the areas are not sore or painful, and give rise to no discomfort. Occasionally, as a ring becomes large, a new one forms at the central parts, and in exceptional cases a patch may show two or three concentric rings. The filiform papillæ are sometimes shed, but the fungiform papillæ may remain and even appear more prominent by reason
1 Literature: Bridou, “Sur une affection innominée de la muqueuse linguale (état lichénoide de M. Gubler),” These de Paris, 1872; Gubler, Dict, encycl. d. Sci. méd., Paris, 1869, vol. i, p. 211, and ibid., 1876, vol. x, p. 234; Alibert, Gaz. des hôp., 1875, P. 806; Caspary, Archiv, 1880, p. 183 (with colored plate); Vanlair, Revue men. de méd. et de Chirurg., 1880, vol. iv, pp. 51 and 227 (with review and some references); Barker, London Path. Soc’y Trans., 188p, vol. xxxi, p. 353, and Holmes and Hulke’s Syst. of Surg., third edit., 1883, ii, p. 560; Gautier, Revue méd. de la suisse romand., 1881, p. 589 (with review and references); Parrot, Progrès méd., 1881, p. 191 (31 cases); Unna, Archiv, 1881, p. 295 (12 cases); Lemonnier, “De la glossite exfoliatrice marginée,” These de Paris, 1883 (with bibliography to date); Colcott Fox, Lancet, 1884, i, p. 842 (10 cases; gives the earliest literature); Butlin, Diseases of the Tongue, 1885; Kaposi, Wien. med. Presse, 1885, p. 361; Guinon, Rev. mens. de mal. de l' enfance, 1887, p. 385 (6 cases); Kinnier, Jour. Cutan. Dis., 1887, p. 56; Hartzell, Med. News, 1887, vol. li, p. 502; Mibelli, Giorn. ital., 1888, p. 383; Molènes, Arch, de laryngol., 1889, vol. ii, p. 326 (full review with bibliography); Bayet, Clinique, Brussels, 1889, vol. iii, p. 657; Besnier, Annales, 1889, p. 320 (case demonstration); Hutchinson, Arch, of Surg., 1892-93, vol. iv, p. 156; Allen, Jour. Cutan. Dis., 1897, p. 159 (case demonstration); Du Castel, Annales, 1897, p. 482 (case demonstration); Colleville, Gaz. hebdom., 1898, p. 277; Mikulicz and Kümmel, Die Krankheiten des Mundes, Jena, 1898, p. 120 (a good illustration); Böhm, Sammlung. klin. Vorträge, Leipzig, 1899, No. 249 (innere Medicin, No. 75), p. 1467 (a clear and exhaustive review); Butlin and Spencer, Diseases of the Tongue, 1900, p. 94 (with colored plate).
TRANSITORY BENIGN PLAQUES OF THE TONGUE 1211
of their isolation (Butlin and Spencer). In most instances there have been practically no subjective symptoms, but itching is occasionally noted, and in Barker’s 2 cases it was quite marked, and associated with increased salivary flow.
Etiology and Pathology.—The malady is rare. It is most frequent in children under the age of two years; Parrot’s 31 cases were under six, Guinon’s 6 under four, Col-cott Fox’s 10 under five. The 2 cases under my own observation were under four. It is, however, seen in older children and also in adults (Vanlair, Lailler, Unna, Hartzell, Besnier, Molènes, Allen, Paget), in the latter much more frequently than formerly thought. Of Unna’s 14 cases, 12 were adults. Hartzell’s patient was aged forty-two, and 1 of Vanlair’s sixty-six. It is met with in both sexes.
The cause of the disease is not known. Parrot looked upon it as syphilis, but his experience was with foundlings, and he was inclined to look upon most obscure affections as of suspicious nature. Fournier is disposed to class it among the indirect consequences of syphilis—among his parasyphilides. Almost all others (Vanlair, Lemonnier, Vidal, Caspary, Besnier, Unna, Du Castel, Molènes, Hartzell, Butlin and Spencer, and others) hold, and properly, I believe, that it is in no way related to syphilis. In my own cases there was not a suspicion of such cause. Moreover, both Unna and Du Castel met with patients who con tracted syphilis after the spots had pre sented. Gastrointestinal disturbance is looked upon (Gubler, Bergeron, Vanlair, Colcott Fox, Molènes, Hartzell, and others) by most observers as of etiologic influence, and such appeared to be of import in my patients. Others, especially Unna, consider it a malady of tropho-neurotic origin. Unna, Barker, and Cas-pary have seen it in delicate children. Spencer’s case developed after scarlet fever, and in Bergeron’s hospital intern during convalescence from typhoid. Besnier views it as a form of eczema, having seen it associated with seborrheic eczema of the integument. The appear ance and manner of spread have sug gested ringworm, and Barker found a fungus in 1 case which both he and Hutchinson thought resembled the trichophyton, but this is the only instance, all others having failed to find any special organism. Kinnier saw these tongue spots as sociated with ringworm patches on the skin. The evanescence and behavior of the areas, as well as their persistent recurrence and the failure to find fungus elements, seem conclusive against this view. A hereditary or family tendency has sometimes been noted; the mother of one of Bridou’s patients had it in childhood; Colcott Fox saw it in a brother and sister; Caspary observed it in 2 instances in two children in the same family; Gubler has seen a whole family affected. In one of Hutchinson’s
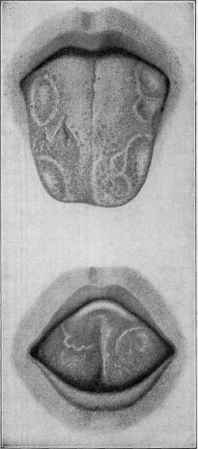
Fig. 330.—Transitory benign plaques of the tongue (Caspary).
1212 SUPPLEMENTARY SECTION
patients the other members of the family had a tendency to sores on the lips and in the mouth.
According to Parrot, the epithelium is found tumefied and thickened, and the cells of the horny and Malpighian layers augmented, those of the latter showing signs of proliferation; lymphoid cells were found in the papillae and about the vessels in the subjacent derma. Unna states it to be an epithelial disease, with its seat quite super ficial in the horny layer.
Diagnosis.—This is a matter of no difficulty, as the superficial character, their well-defined outline, with the reddish, sometimes desquamating, central portion, and the usually grayish or yellowish border, when taken together with the history, the rapidity of their formation, capriciousness, and recurrence, will serve to differentiate from syphilitic mucous patches, aphthæ, and leukoplakia.
Prognosis and Treatment.—The malady, while benign, is generally persistent, although in children it seems, in most instances, to tend to spontaneous disappearance as they grow older. It is ordinarily rebellious to treatment, although a careful super vision of the dietary and the maintenance of good digestion and free action of the bowels will often have a material influence. In feeble subjects tonics and cod-liver oil may be of service. Hartzell found in his case arsenic, also commended by Vanlair and Brocq, lengthened the intervals between the attacks. Mildly astringent and antiseptic mouth washes are commonly prescribed. Besnier advises applications of boric acid ointment made with vaselin and with the addition of balsam’ of Peru. Unna states that he has had most satisfaction from sulphur applications. The most convenient for this purpose is, as Bénard suggests, the natural sulphur water, although Unna employs emulsive liquids containing washed sulphur. In my 2 cases the most benefit seemed derived from attention to digestion and the occasional administration of a laxa tive of antacid, such as calcined magnesia, together with a myrrh and boric acid mouth-wash.
BLACK TONGUE1
Synonyms.—Hairy tongue; Lingua nigra; Hyperkeratosis linguae; Fr., Langue noire; Nigritie de la langue; Hypertrophie épithéliale filiforme; Langue noire pileuse; Ger., Haarzunge; Schwarze Haarzunge.
This curious malady is rare, although probably not so much so as commonly be lieved, inasmuch as it practically gives rise to no trouble, and sooner or later passes away spontaneously. The usual situation is immediately in front of the circumvallate papillae, although exceptionally on other parts of the tongue; in Curtis’ patient the patch was behind these papillae, and in Lediard’s and Eve’s near the end, and in Lake’s at the left side, middle third. The color is generally black, but in an instance observed
1 Literature: Dessois, De la langue noire (Glossophytie), Paris, 1878; Hutchinson, Med. Press and Circular, 1883, ii, p. 20; Stokes, London Path. Soc’y Trans., 1884, vol. xxxv, p. 157; Lediard, ibid., 1886, vol. xxxvii, p. 222 (brief note); Roth, Wien. med. Presse, 1887, pp. 935 and 987 (2 cases); Brosin, “Ueber die schwarze Zunge,” Ham burg and Leipzig, 1888, Ergänzungsheft, Monatshefte, 1888 (with illustration, review, and analytic table of cases (23) to date, with references); Curtis, New York Med. Jour., 1889, vol. 1, p. 216 (case demonstration); Leviseur, ibid., 1889, vol. xlix, p. 42; Lake, Brit. Med. Jour., 1891, ii, p. 946; Smith, ibid., p. 1043 (letter communication—2 cases); Masters, ibid.; Rydygier, Arch, fur klin. Chirurg., 1891, vol. xli, p. 767 (with illustration); Ciaglinski and Hewelke, Zeitschr. für klin. Med., 1893, vol. xxii, p. 626 (with review and bibliography); Mourek, Archiv, 1894, vol. xxix, p. 369; Sendziak, Rev. de laryng., otol., et de rhinol., 1894, vol. xiv, p. 228, and (same paper) Monats-hefle fur Ohrenheilk., 1894, vol. xxviii, p. 112 (with review and references); Goodale, Jour. Boston Soc. Med. Sci., 1897-98, ii, p. 204 (histology); Vollmer, Archiv, 1898, vol. xlvi, p. 12 (histology, with illustrations); Gottheil, Arch. Pediat., 1899, p. 255 (with illustration of case and fungus found); Heidingsfeld, Jour. Amer. Med. Assoc, Dec 17, 1910, p. 2117 (report of 2 cases; histology with illustrations, review, and bib liography).
BLACK TONGUE 1213
by Dinkier it was yellow, and one by Mourek, blue. The area forms gradually, as a rule, centrally, and extends peripherally; the reverse takes place in its disappearance. In some instances (Curtis, Ciaglinski and Hewelke, Masters, Lake), however, it de velops rapidly, occupying considerable area in from several days to one or two weeks. The condition may consist simply of discoloration (Stokes, Ciaglinski and Hewelke, Sendziak, Gottheil), or, as usually observed, beset with thin, filiform projections, also dark colored or black, which may be likened in appearance to long tendrils, lashes, sea weed (Curtis), or hairs; so much like the last in many instances that they were suspected of being true hairy growths, hence the term “hairy tongue.” In some cases, as Raynaud (cited by Lake) expressed it, the area looks like “a field of corn laid by wind and storm.” These filiform projections can reach considerable length. With the exception some times of a mawkish taste when the patch is well developed, there are practically no troublesome subjective symptoms; rarely slight pain, although in Curtis’ case this was quite pro nounced.
The causes are not known. Syphilis has been suggested as possibly causative, but beyond the fact that it has occasionally been seen (Leviseur, Vollmer) in those who have had this disease there is nothing to support this view. It is not impos sible that the resulting stomatitis from mercurial treatment, the use of irritating mouth-washes, ex cessive smoking, etc., may have some influence in its production. The malady is seen in children and adults, in the former with usually but little, and frequently no, filiform projections. In adults it may also sometimes consist practically of pig mentation alone, but commonly shows variable filiform or hair-like formations also. Its occur rence in one instance observed by Röstowjew1 in man and wife suggested to this observer the possi bility of contagiousness. It occurs in both sexes, but reaches its greatest “hairy” development in male adults. The projecting filaments consist of enormously lengthened filiform papillae produced by a hyperkeratosis or overgrowth of the epidermis of these papillae; the edges are usually serrated from imbrication of their investing epithelium. Sometimes these elongated, soft, and wavy or stiff hair-like formations show lateral projections, so strikingly, as in Goodale’s patient, as to suggest the comparison to a feather with stem and lateral webs. A reason for this excessive hyperkeratosis is hard to find. Heidingsfeld found that “the fundamental abnormality is the presence of abnormal papillae and interpapillary processes or filament founts, situated within the epidermis from which the abnormally elongated, stratified, and kera-tosed filaments trace their direct origin.” The malady has been thought probably due to parasitic influence, and various observers have discovered organisms, but several, and sometimes numbers, are to be found on the tongue, even when this organ is free from disease. The spore-like bodies which Gottheil and Heidingsfeld detected were probably similar to those reported by Dessois, Laveau, Lancereaux, Schech, Gubler, and others. That which Ciaglinski and Hewelke and Sendziak found and cultivated was a black mold consisting of a stalk-like formation having spheric capsules on the end containing black spores; a mushroom-shaped columella developed from the burst spore capsule. Many investigators, however, have failed to corroborate these and other findings reported. It is probable that the color is due to chromatogenous organ isms, although this is by no means proved. Goodale attributed the color in his case 1 Röstowjew, abs. in Monatshefte, 1899, vol. xxiv, p. 41.

Fig. 331.—Black tongue, show ing the filamentous or hair-like development.
1214
SUPPLEMENTARY SECTION
to highly refractile, yellowish-brown granules. Hutchinson was inclined to believe that in his patient (pigmentation only) the color was purposely produced.
Prognosis and Treatment.—The malady is somewhat variable in its behavior in different cases. It may persist for several weeks, months, or years, and then gradu ally or quickly spontaneously disappear; or, as in Stokes’ patient, practically of pig mentation only, the blackness fluctuates in degree and extent. Treatment seems to be of little avail. Shaving and scraping, sometimes practised, will remove the filiform formations, but regrowth usually occurs. Exfoliation can, if thought advisable, be pro duced by the resorcin peeling paste, by solutions of salicylic acid and weakened lactic acid. Upon the whole, except as to the maintenance of cleanliness, the applications of mild antiseptics and astringents, such as glycerite of tannic acid, the malady is best let alone. It generally disappears spontaneously sooner or later.
CHEILITIS GLANDULARIS
Synonyms.—Cheilitis glandularis apostematosa (Volkmann); Myxadenitis labialis.
Volkmann1 was the first to describe this rare malady, his cases being character ized by chronic inflammation of the lower lip, chiefly of the vermilion part, but extend ing on to the mucous membrane proper, as well as occasionally involving the adjacent skin; the latter was erythematous in appearance. The lip becomes somewhat tense and swollen, and the mucous glands prominent, being the size of a hemp-seed or larger, with follicular openings much dilated, sufficiently marked in some instances to permit the introduction of a fine probe. An opaque mucous or mucopurulent secretion readily

Fig. 332.—Cheilitis glandularis (courtesy of Dr. Richard L. Sutton).
exuded upon slight pressure, and there was variable spontaneous oozing, which tended now and then to form more or less crusting. It is not uncommon for the lips to be glued together in the morning. Some of the openings were of a fistulous character, in 1 case as many as 10 to 15 being found in the inside of the lip, admitting a large probe, and forming irregular, fistulous tracts. Furuncle- and abscess-like inflammatory for mations sometimes developed in the fleshy part of the lip, but actual ulcerative action, Volkmann states, did not occur.
Purdon2 has met with 4 examples of the same malady, all adults—3 males and 1 female. The disease was confined in 3 patients to the lower lip and its mucous lining, beginning gradually, and spreading over the entire surface of the lip. The mucous glands of the lip were swollen, and could be felt with the finger, often as nodular masses. These conditions were most pronounced during exacerbations, at such times the lip becoming tense, swollen, and hard, and, as in Volkmann’s cases, with mobility more or less impaired. A turbid and mucopurulent secretion was pressed out of these glands, the ducts of which were dilated. In fact, there seemed, Purdon states, to be also an
1 Volkmann, Virchow's Archiv, 1870, vol. 1, p. 142 (5 cases).
2 Purdon, Brit. Jour. Derm., 1893, p. 23 (4 cases).
FORDYCE’S DISEASE 1215
active catarrhal condition of the lining membrane of the cheeks and gums. There were no fistulous tracts as in some of Volkmann’s patients. In 1 patient both lips were affected, and frequently found glued together in the morning. In 1 case the skin of the chin became erythematous. Sutton1 has reported 3 American cases more or less typical.
The cause of the malady is not known. It is entirely distinct from cheilitis ex-foliativa, a more common affection, with constant and persistent exfoliation and crust accumulation as its chief feature. The patients seemed otherwise in good health. The etiologic factor is to be sought for in the catarrhal condition of the mouth and pharynx, the mucous glands of the lip becoming subsequently involved. It is not syphilitic. It usually begins in early or middle adult life. Sutton’s histologic study indicates that the disease is an adenomatous condition of the mucous glands of the lip characterized by enormous dilatation and hypertrophy of ducts, usually accompanied by a great increase in the amount of glandular tissue.
Prognosis and Treatment.—The malady is persistent and rebellious to treatment.2 Volkmann cured 3 of his cases in one to two months with potassium iodid internally, gargles of potassium chlorate, and mild cauterization of the parts with silver nitrate. Purdon was not so successful, the disease seeming obstinate to all remedies. What gave most benefit was the local application of lotio nigra and glycerin, with occasional penciling with silver nitrate solution; x-ray treatment was found promising in Sutton’s cases.
FORDYCE’S DISEASE
Synonym.—Fordyce’s disease of the lips and oral mucous membrane.
The first description of this peculiar affection, involving the vermilion of lips and mucous membrane of the mouth, we owe to Fordyce (1896).3 Since then the same condition has been observed by Montgomery and Hay, Audry, Delbanco, Heuss, Allen, White, and others.4 It is characterized by the appearance of whitish or yellowish, scanty or abundant, discrete, aggregated, and often practically coalescent, milium-
1 Sutton, Jour. Cutan. Dis., 1909, p. 151 (with case illustration, case report and review of the literature, with references), and Unna-Festschrift, Band 1, p. 611; 2 addi tional American cases (with case and histologic illustrations; review and references); Howard Fox, Jour. Cutan. Dis., 1909, p. 229 (case presentation—patient born in Ire land); Schamberg, Jour. Cutan. Dis., 1911, p. 449 (case demonstration; man aged forty-four, involving lower lip, of two years’ duration).
2 Unna, “Ueber Erkrankungen der Schleimdrüsen des Mundes,” Monatshefte, 1890, vol. xi, p. 317, reports several cases of a malady (Baelz’s disease) in many respects apparently similar, and to which his attention had been previously called by Baelz; the lip, usually the under lip only, was involved, and with the early symptoms above described, but the mucous glandular swelling went on to pronounced suppuration, crust ing, and ulceration, and then cicatrization; he found that local treatment with tinc ture of iodin, a plan pointed out to him by Baelz, acted as a specific, improvement ensuing immediately; Jamieson (Brit. Med. Jour., Dec 7,1895 (cited by Fordyce)) has reported a case apparently similar to those described by Unna.
3 Fordyce, “A Peculiar Affection of the Mucous Membrane of the Lips and Oral Cavity,” Jour. Cutan. Dis., 1896, p. 413 (with colored plate, case illustration, and histologic cuts).
4 D. W. Montgomery and Hay, “Sebaceous Glands in the Mucous Membrane of the Mouth,” Proceedings of the Tenth Annual Sessions of the Assoc. Amer. Anatomists,
1897, p. 76; Audry, “Ueber eine Veränderung der Lippen- und Mundschleimhaut bestehend in der Entwickelung atrophischer Talgdrüsen,” Monatshefte, 1899, vol. xxix, p. 101 (with histologic plate); Delbanco, “Ueber die Entwichelung von Talgdrüsen in der Schleimhaut des Mundes,” ibid., pp. 104 and 353, and Münch, med. Wochenschr.,
1898, p. 1510 (case demonstration), and ibid., 1899, p. 459 (case demonstration); Heuss, “Ueber postembryonale Entwickelung von Talgdrüsen in der Schleimhaut der mensch-lichen Mundhöhle,” ibid., 1900, vol. xxxi, p. 501 (with review); Allen, Jour. Cutan. Dis., 1897, p. 29 (case demonstration); Suchannek, “Ueber gehäuftes Vorkommen von Talgdrüsen in der menschlichen Mundschleimhaut,” Munch, med. Wochenschr., 1900, i, P. 575.
1216 SUPPLEMENTARY SECTION
like bodies, occurring more especially on the inside of the mouth, laterally along the line of the teeth as far back as the last molar, and possibly somewhat less frequently on the vermilion or mucous and inner surface of the lips. There is but slight elevation, but they are more projecting on the oral membrane than on the lips. The color of the formations in the mouth are also more of the white, with the yellow or yellowish aspect less pronounced than observed in the lip lesions. When numerous and closely crowded,
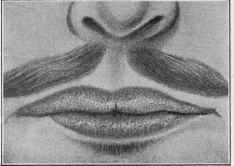
Fig. 333—Fordyce’s disease; lesions are closely crowded (courtesy of Dr. J. A. Fordyce).
the appearance of a solid, yellowish patch is presented, but the constituent, milium-like bodies can be readily discovered or rendered much more conspicuous by putting the tissues on the stretch. As a rule there are no subjective symptoms, although occasion ally in some instances a feeling of slight burning and itching, accompanied by some stiff ness as though the lip were swollen (Fordyce).
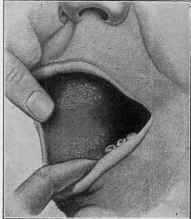
Fig. 334.—Fordyce’s disease, showing lesions in the mouth (Delbanco).
Etiology and Pathology.—The condition is not, as at first thought, very rare, but, owing to its comparatively insignificant character, relatively few individuals af fected seek advice. It is seen most frequently in male adults. In 12 cases investi gated by Heuss, in a number of which the lesions were in the oral cavity and scanty, the patients were aged between twenty-five and fifty, and there were only 3 women. Montgomery and Hay and Audry saw the development in 1 instance in an infant. Fordyce’s patient (a physician) found the lesions in all other members of his family, but they appeared after puberty; he also found them in “half of the negroes examined."
LA PERLECHE 1217
The formations have been histologically investigated by Fordyce, Montgomery and Hay, Delbanco, Heuss, and White. Fordyce first thought they were due to a granu lar change in the protoplasm of the cells of the affected mucous membrane, but subsequently agreed with the observations by the others named that they are in reality slightly or moderately, sometimes markedly, developed sebaceous glands. Montgomery and Hay were, by their investigations of these peculiar bodies, the first to show that these glandular structures are sometimes to be found in the mucous membrane of the oral cavity. C. J. White,1 in still later investigations, claims that Fordyce’s original opinion is the correct one, as he found that the sebaceous element, though abundantly present, lies beyond the diseased tissue proper.
There is some difference of opinion as to whether these glands are simply a late development of pre-existing embryonic elements (Audry), or whether they are purely postnatal in origin (Heuss). This latter observer believes their growth and develop ment are favored by catarrhal conditions, stomatitis, etc, and thinks that their appar ent greater prevalence in those who have had syphilis is due to the stomatitis which the mercurial treatment sometimes causes. They have, of course, as all observers agree, no direct connection with syphilis, and it is more than probable that in the cases in vestigated (Montgomery and Hay, Delbanco, Heuss), in which syphilis had previously existed, their presence was purely a matter of coincidence.
Prognosis and Treatment.—The condition, while benign, is persistent, and shows but little, if any, tendency toward retrogressive changes, although in a few instances the lesions became, in course of time, smaller and less conspicuous. Treatment has not been satisfactory. Fordyce found that when the superficial layer of the epithelium was scraped away, some of the bodies could be pressed out, and the discoloration thus somewhat lessened; the effect was, however, only temporary.
LA PERLECHE
Synonyms.—Bridou; Parasitic disease of the lips.
This is a peculiar affection of the lips, especially of the commissures, observed chiefly in certain districts of France, and first clearly described by Lemaistre,2 and since by Raymond,3 Guibert,4 Planche,5 and a few others. It occurs almost exclusively in infants and young children. It begins, as a rule, in the angles, bilaterally, first pre senting as a blanching of the epithelium and having a somewhat sodden appearance. It extends to a variable distance along the vermilion surface toward the median line, but usually only part way, in some instances invading the neighboring skin, and in most cases the mucous membrane of the inside of the lips as well. There is frequently some underlying and surrounding hyperemia and inflammation, and the mouth-angles are sometimes crusted over. Other parts of the inside of the mouth may also show in volvement. In a large number of cases the disease remains limited to the angles of the mouth and the immediately adjacent parts. On the true mucous surface, and also in a great measure at the commissures, the appearances presented are somewhat like those of syphilitic mucous patches. There is a distinct tendency at the com missures of the mouth to the formation of a deep fissure, with often smaller ones nearby, and with a disposition sometimes to bleeding. The epithelium of the lips becomes
1 C. J. White, Jour. Cutan. Dis., March, 1905, p. 97 (a report of 65 cases, with histologic cuts and a complete review of the subject, and literature with bibliography).
2 Lemaistre, “Etude sur l'air de la ville de Limoges; de la perlèche; du strepto coccus plicatilis,” Jour. soc. de méd. et de la pharm. de la Haute-Vienne, Limoges, 1886, pp. 41, 55, and 74.
3 Raymond, “Etude clinique et bactériologique sur la perlèche," Annales, 1893, P. 578.
4 Guibert, “De la perlèche,” These, No. 142, Toulouse, 1896.
5 Planche, “La Perlèche,” These de Paris, 1897; Négrié, “Note sur la perlèche,” Cong, de Gynecol. d’obstet. et de pêdiat., first session, Bordeaux, Aug., 1895, p. 1002.
77
1218 SUPPLEMENTARY SECTION
slightly thickened, macerated, and more or less readily detachable. The condition is aggravated by the child frequently moistening the parts with the tongue in attempts to relieve the dryness and parched and burning feeling. There is also sometimes itching.
The malady is contagious, and spreads quite rapidly in maternity hospitals, found ling and infant asylums, and among young schoolchildren (see Lemaistre and Ray-mond’s papers). It is thought to be conveyed through the medium of the water-sup ply, drinking-cups and spoons, and other utensils. According to Lemaistre, it is due to an organism named by him Streptococcus plicatilis. Raymond, on the other hand, attributes it chiefly to the Staphylococcus cereus albus, although admitting that it may be produced by various other organisms, and that the malady usually starts from the inside of the lips. This opinion is also shared by Guibert and Planche. Sa-bouraud believes it may result from a streptococcic salivary infection or be associ ated with a streptococcic impetigo. The resemblance to the mucous patch and fissures of syphilis is at times so striking that these several observers agree that in some cases the presence or absence of other symptoms of syphilis must be the determining factor in the differential diagnosis. Raymond considers the diphtheroid-looking spots some times seen in the mouths of infants and young children practically the same disease.
Prognosis and Treatment.—The affection generally runs its course in from a few weeks to one or two months, with sometimes a marked disposition to relapse. Treat ment consists in frequent cleansing and the occasional application of a weak solution of silver nitrate, copper sulphate, or alum, together with mild ointments or such other remedies as may be indicated. Attention is to be given to the nursing-bottles, drink-ing-vessels, water-supply, etc.
But first, if you want to come back to this web site again, just add it to your bookmarks or favorites now! Then you'll find it easy!
Also, please consider sharing our helpful website with your online friends.
BELOW ARE OUR OTHER HEALTH WEB SITES: |
Copyright © 2000-present Donald Urquhart. All Rights Reserved. All universal rights reserved. Designated trademarks and brands are the property of their respective owners. Use of this Web site constitutes acceptance of our legal disclaimer. | Contact Us | Privacy Policy | About Us |